

Comprehensive Human Papillomavirus Genotyping in Cervical Squamous Cell Carcinomas and Its Relevance to Cervical Cancer Prevention in Malawian Women
- PMID: 28717764
- PMCID: PMC5493214
- DOI: 10.1200/JGO.2015.001909
Comprehensive Human Papillomavirus Genotyping in Cervical Squamous Cell Carcinomas and Its Relevance to Cervical Cancer Prevention in Malawian Women
Abstract
Purpose: Cervical squamous cell carcinoma (SCC) continues to be a significant cause of cancer morbidity and is the third leading cause of cancer-related death in women worldwide. In sub-Saharan Africa, cervical cancer is not only the most common female cancer but also the leading cause of cancer-related deaths in women. Malawi, in particular, has the highest burden of cervical cancer. With the increasing use of human papillomavirus (HPV) vaccination, documenting the prevalent HPV types in those high-risk populations is necessary to both manage expectations of HPV vaccination and guide future vaccine development.
Materials and methods: In this study, we performed HPV typing on 474 cervical SCC samples and analyzed the potential impact of HPV vaccination in this population.
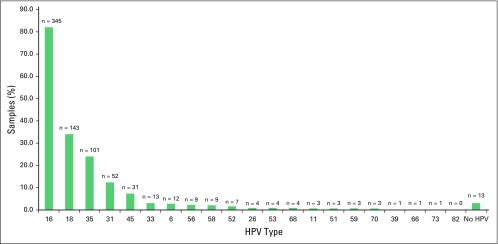
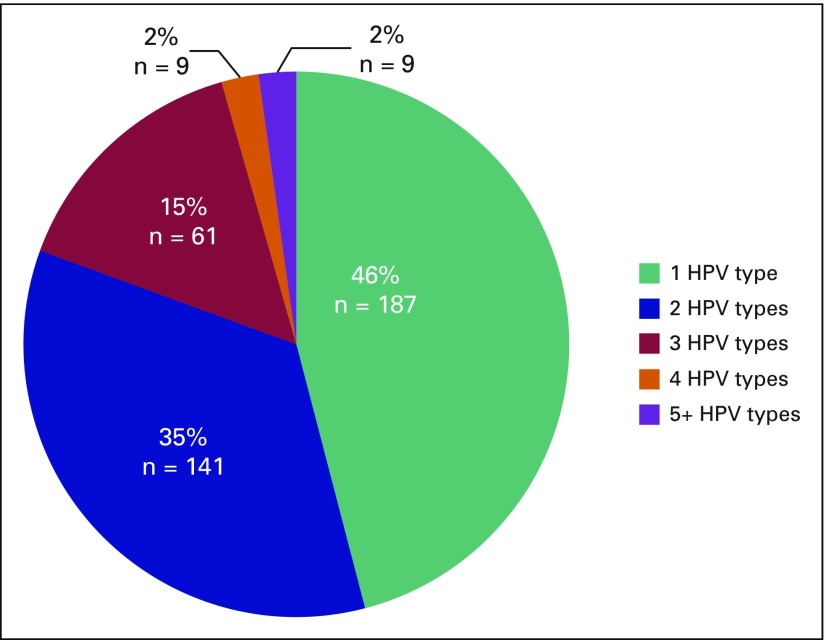
Results: Ninety-seven percent of tumors were positive for at least one HPV type, and 54% harbored more than one HPV type. HPV 16 was the most common type (82%), followed by HPV 18 (34%), HPV 35 (24%), and HPV 31 (12%). A vaccine against HPV 16 and 18 would ideally prevent 53% of cervical SCC, and the nonavalent HPV vaccine (covering HPV 16, 18, 31, 33, 45, 52, and 58) would prevent 71% of cervical SCC in Malawi (assuming 100% vaccine efficacy). The main reason for a lack of coverage was high prevalence of HPV 35, which was also present as a single infection in a small subset of patients.
Conclusion: Although any HPV vaccination in this population would likely prevent a significant proportion of cervical cancer, the nonavalent vaccine would provide better coverage. Furthermore, investigation of the role of HPV 35 in this population, including possible cross-protection with other HPV types, should be pursued.
Conflict of interest statement
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/site/ifc. Brooke E. HowittNo relationship to discloseMichael HerfsNo relationship to discloseTamiwe TomokaNo relationship to discloseSteve KamizaNo relationship to discloseTarik GheitNo relationship to discloseMassimo TommasinoNo relationship to disclosePhilippe DelvenneNo relationship to discloseChristopher P. CrumNo relationship to discloseDanny MilnerNo relationship to disclose
Figures
Similar articles
-
Impact of high-risk Human Papillomavirus genotyping in cervical disease in the Northern region of Portugal: Real-world data from regional cervical cancer screening program.J Med Virol. 2023 Jan;95(1):e28414. doi: 10.1002/jmv.28414. J Med Virol. 2023. PMID: 36541747
-
Genotype prevalence and age distribution of human papillomavirus from infection to cervical cancer in Japanese women: A systematic review and meta-analysis.Vaccine. 2022 Sep 29;40(41):5971-5996. doi: 10.1016/j.vaccine.2022.07.052. Epub 2022 Sep 6. Vaccine. 2022. PMID: 36085257
-
The Clinical and Economic Impact of a Nonavalent Versus Bivalent Human Papillomavirus National Vaccination Program in Taiwan.Value Health Reg Issues. 2022 Nov;32:79-87. doi: 10.1016/j.vhri.2022.06.006. Epub 2022 Sep 15. Value Health Reg Issues. 2022. PMID: 36116338
-
Public health impact and cost-effectiveness of switching from bivalent to nonavalent vaccine for human papillomavirus in Norway: incorporating the full health impact of all HPV-related diseases.J Med Econ. 2023 Jan-Dec;26(1):1085-1098. doi: 10.1080/13696998.2023.2250194. J Med Econ. 2023. PMID: 37608730
-
Comparison of different human papillomavirus (HPV) vaccine types and dose schedules for prevention of HPV-related disease in females and males.Cochrane Database Syst Rev. 2019 Nov 22;2019(11):CD013479. doi: 10.1002/14651858.CD013479. Cochrane Database Syst Rev. 2019. PMID: 31755549 Free PMC article.
Cited by
-
Whole-Genome Analysis of Cervical Human Papillomavirus Type 35 from rural Zimbabwean Women.Sci Rep. 2020 Apr 24;10(1):7001. doi: 10.1038/s41598-020-63882-z. Sci Rep. 2020. PMID: 32332798 Free PMC article.
-
Prevalence of human papillomavirus genotypes in cervical cancer in Maiduguri, Nigeria.Pan Afr Med J. 2019 Aug 5;33:284. doi: 10.11604/pamj.2019.33.284.18338. eCollection 2019. Pan Afr Med J. 2019. PMID: 31692869 Free PMC article.
-
Community-based self-collected human papillomavirus screening in rural Zimbabwe.BMC Public Health. 2019 May 29;19(Suppl 1):603. doi: 10.1186/s12889-019-6810-5. BMC Public Health. 2019. PMID: 31138174 Free PMC article.
-
Human papillomavirus type-specific distribution in cervical intraepithelial neoplasia and cancer in The Gambia prior to HPV immunization programme: a baseline for monitoring the quadrivalent vaccine.Infect Agent Cancer. 2024 Sep 12;19(1):44. doi: 10.1186/s13027-024-00601-7. Infect Agent Cancer. 2024. PMID: 39267099 Free PMC article.
-
Human papillomavirus genotype distribution patterns in Zimbabwe; is the bivalent vaccine sufficient?Intervirology. 2024 Apr 4;67(1):55-63. doi: 10.1159/000531347. Online ahead of print. Intervirology. 2024. PMID: 38574482 Free PMC article. Review.
References
-
- Ferlay J, Shin HR, Bray F, et al. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127:2893–2917. - PubMed
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136:E359–E386. - PubMed
-
- Denny L, Adewole I, Anorlu R, et al. Human papillomavirus prevalence and type distribution in invasive cervical cancer in sub-Saharan Africa. Int J Cancer. 2014;134:1389–1398. - PubMed
-
- Louie KS, de Sanjose S, Mayaud P. Epidemiology and prevention of human papillomavirus and cervical cancer in sub-Saharan Africa: A comprehensive review. Trop Med Int Health. 2009;14:1287–1302. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
