

Multimodality Image-Guided Cryoablation for Inoperable Tumor-Induced Osteomalacia
- PMID: 28718983
- PMCID: PMC5685881
- DOI: 10.1002/jbmr.3219
Multimodality Image-Guided Cryoablation for Inoperable Tumor-Induced Osteomalacia
Abstract
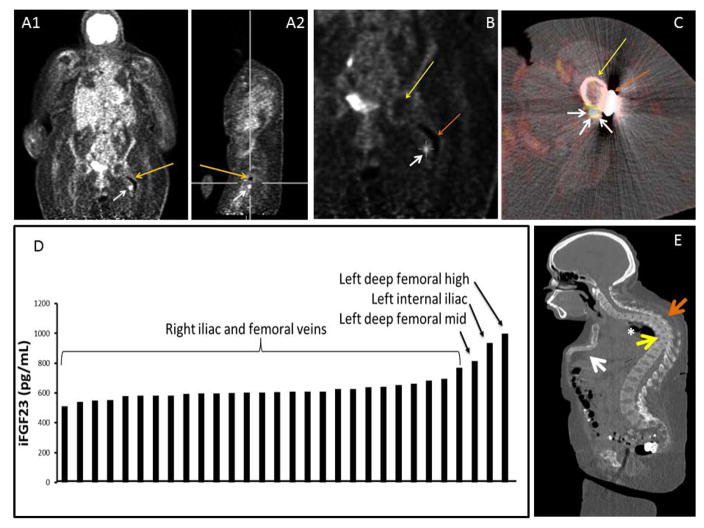
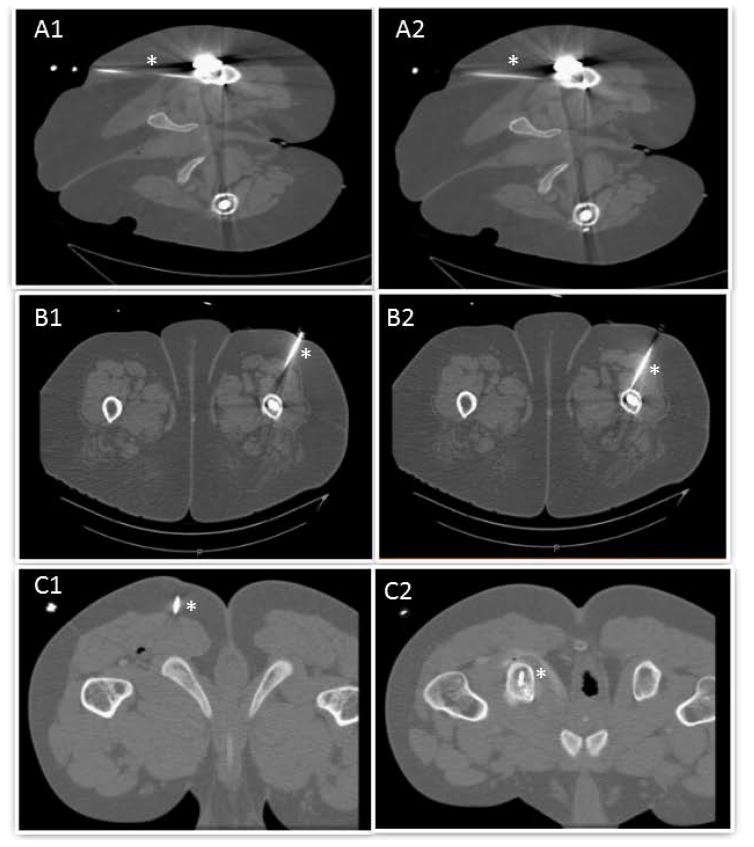
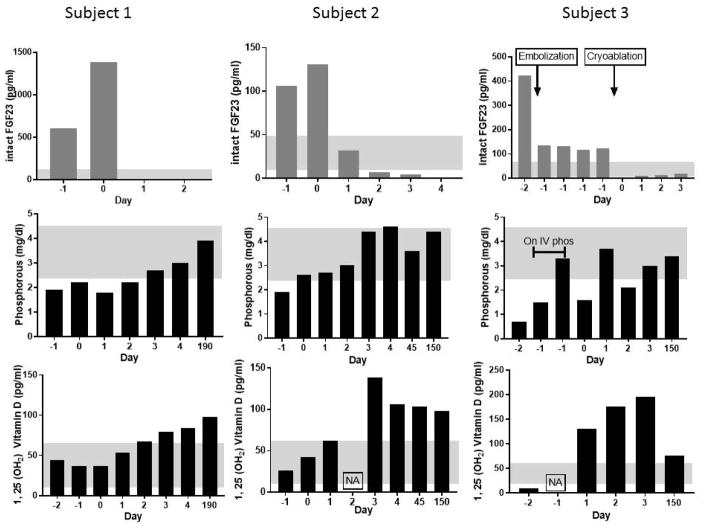
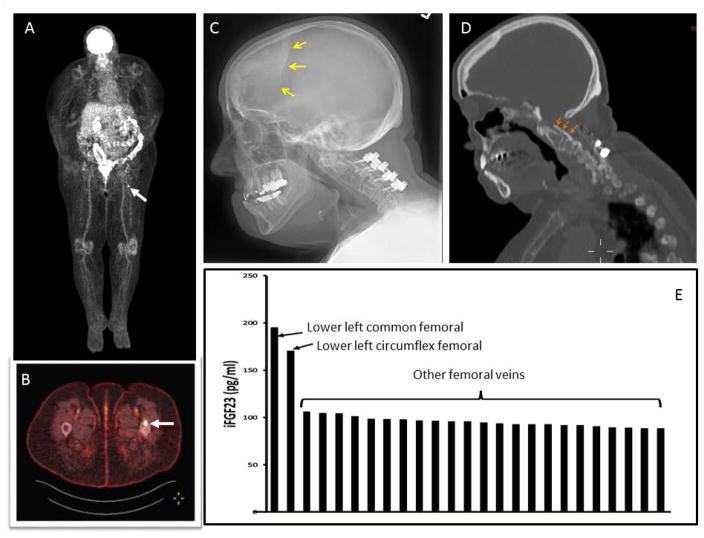
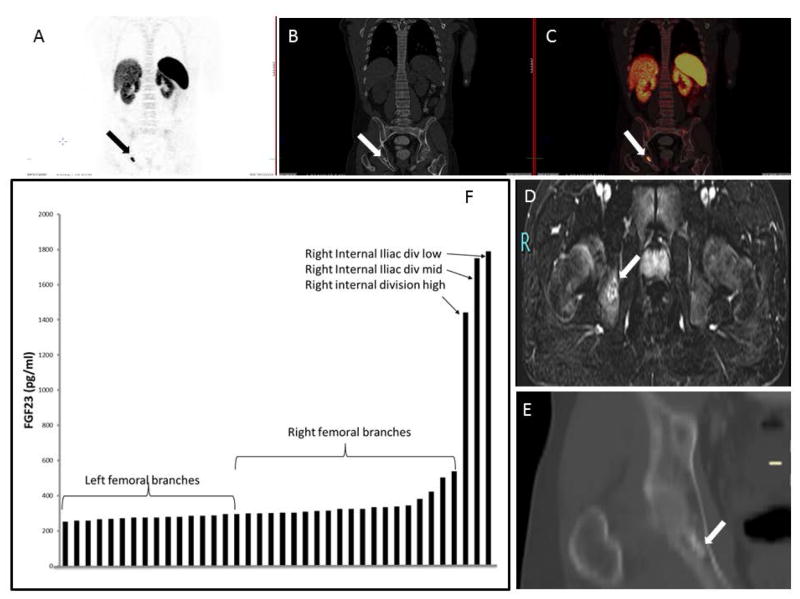
Tumor-induced osteomalacia (TIO) is a debilitating paraneoplastic condition caused by small phosphaturic mesenchymal tumors (PMTs) that secrete large amounts of the phosphate-regulating and vitamin D-regulating hormone, FGF23. Tumor removal results in cure. However, because of high perioperative comorbidity, either from tumor location or host factors, surgery is sometimes not an option. Tumor destruction via cryoablation may be an effective option for inoperable PMTs. Three subjects with a confirmed diagnosis of TIO were studied. All three underwent cryoablation of suspected PMTs rather than surgery due to significant medical comorbidities or challenging anatomical location. Subject 3 had tumor embolization 24 hours prior to cryoablation because of the size and hypervascularity of the tumor. The success of the tumor cryoablation was defined by normalization of serum phosphate and FGF23. Cryoablation resulted in a rapid decrease in plasma intact FGF23 by 24 hours postprocedure in all three subjects (0, 2, and 9 pg/mL, respectively) with normalization of blood phosphate by postprocedure day 3. Three-day renal tubular reabsorption of phosphate increased to 76%, 94%, and 95.2%, respectively; 1, 25(OH)2 vitamin D increased to 84, 138, and 196 pg/ml, respectively. All three had dramatic clinical improvement in pain and weakness. Two subjects tolerated the procedure well with no complications; one had significant prolonged procedure-related localized pain. Although surgery remains the treatment of choice, cryoablation may be an effective, less invasive, and safe treatment for patients with difficult to remove tumors or who are poor surgical candidates. © 2017 American Society for Bone and Mineral Research.
Keywords: CRYOABLATION; FGF23; TIO; TUMOR-INDUCED OSTEOMALACIA.
© 2017 American Society for Bone and Mineral Research.
Figures
References
-
- Shimada T, Hasegawa H, Yamazaki Y, Muto T, Hino R, Takeuchi Y, et al. FGF-23 is a potent regulator of vitamin D metabolism and phosphate homeostasis. J Bone Miner Res. 2004 Mar;19(3):429–35. - PubMed
-
- Chu KF, Dupuy DE. Thermal ablation of tumours: biological mechanisms and advances in therapy. Nature reviews Cancer. 2014 Mar;14(3):199–208. Epub 2014/02/25. - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
