

Pancreatic allograft thrombosis: Suggestion for a CT grading system and management algorithm
- PMID: 28719059
- PMCID: PMC5763322
- DOI: 10.1111/ajt.14433
Pancreatic allograft thrombosis: Suggestion for a CT grading system and management algorithm
Abstract
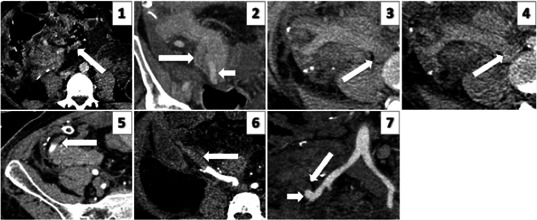
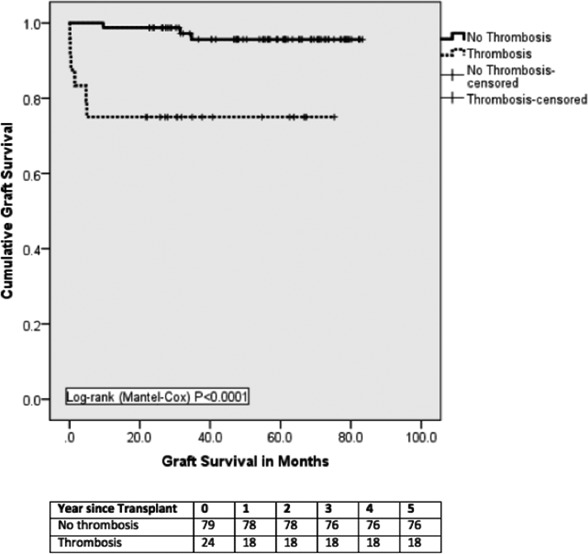
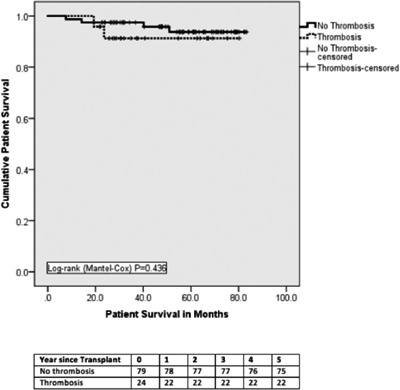
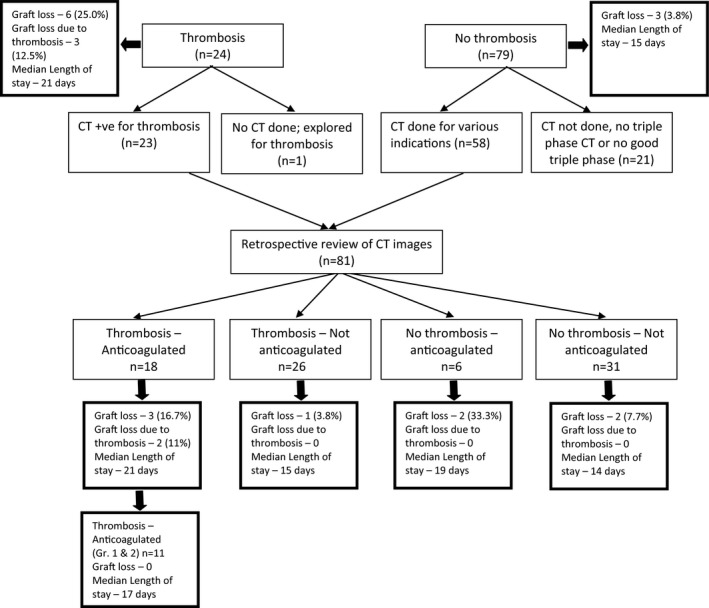
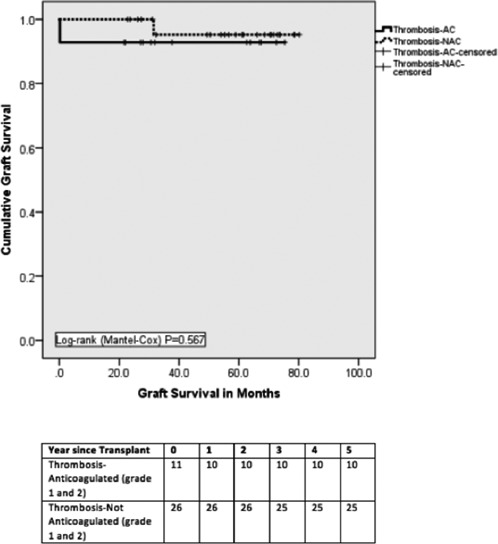
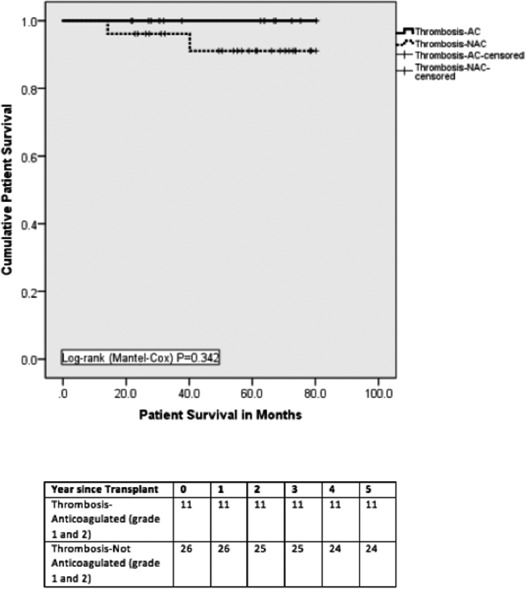
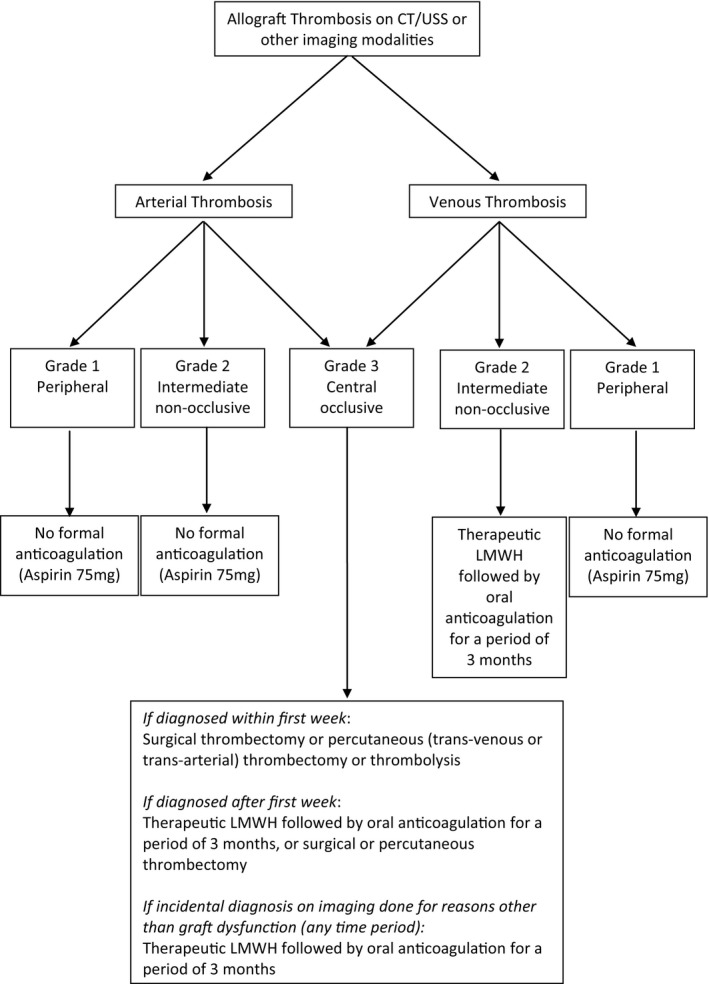
Pancreatic allograft thrombosis (PAT) remains the leading cause of nonimmunologic graft failure. Here, we propose a new computed tomography (CT) grading system of PAT to identify risk factors for allograft loss and outline a management algorithm by retrospective review of consecutive pancreatic transplantations between 2009 and 2014. Triple-phase CT scans were graded independently by 2 radiologists as grade 0, no thrombosis; grade 1, peripheral thrombosis; grade 2, intermediate non-occlusive thrombosis; and grade 3, central occlusive thrombosis. Twenty-four (23.3%) of 103 recipients were diagnosed with PAT (including grade 1). Three (2.9%) grafts were lost due to portal vein thrombosis. On multivariate analysis, pancreas after simultaneous pancreas-kidney transplantation/solitary pancreatic transplantation, acute rejection, and CT findings of peripancreatic edema and/or inflammatory change were significant risk factors for PAT. Retrospective review of CT scans revealed more grade 1 and 2 thromboses than were initially reported. There was no significant difference in graft or patient survival, postoperative stay, or morbidity of recipients with grade 1 or 2 thrombosis who were or were not anticoagulated. Our data suggest that therapeutic anticoagulation is not necessary for grade 1 and 2 arterial and grade 1 venous thrombosis. The proposed grading system can assist clinicians in decision-making and provide standardized reporting for future studies.
Keywords: clinical research/practice; coagulation and hemostasis; complication; graft survival; health services and outcomes research; pancreas/simultaneous pancreas-kidney transplantation; thrombosis and thromboembolism.
© 2017 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Farney AC, Rogers J, Stratta RJ. Pancreas graft thrombosis: causes, prevention, diagnosis, and intervention. Curr Opin Organ Transplant. 2012;17(1):87‐92. - PubMed
-
- Ramessur Chandran S, Kanellis J, Polkinghorne KR, Saunder AC, Mulley WR. Early pancreas allograft thrombosis. Clin Transplant. 2013;27(3):410‐416. - PubMed
-
- Muthusamy AS, Giangrande PL, Friend PJ. Pancreas allograft thrombosis. Transplantation. 2010;90(7):705‐707. - PubMed
-
- Burke GW 3rd, Ciancio G, Figueiro J, et al. Hypercoagulable state associated with kidney‐pancreas transplantation. Thromboelastogram‐directed anti‐coagulation and implications for future therapy. Clin Transplant. 2004;18(4):423‐428. - PubMed
-
- Shahrestani S, Webster AC, Lam VW, et al. Outcomes from pancreatic transplantation in donation after cardiac death: a systematic review and meta‐analysis. Transplantation. 2017;101(1):122‐130. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
