

Human immunology studies using organ donors: Impact of clinical variations on immune parameters in tissues and circulation
- PMID: 28719147
- PMCID: PMC5740015
- DOI: 10.1111/ajt.14434
Human immunology studies using organ donors: Impact of clinical variations on immune parameters in tissues and circulation
Abstract
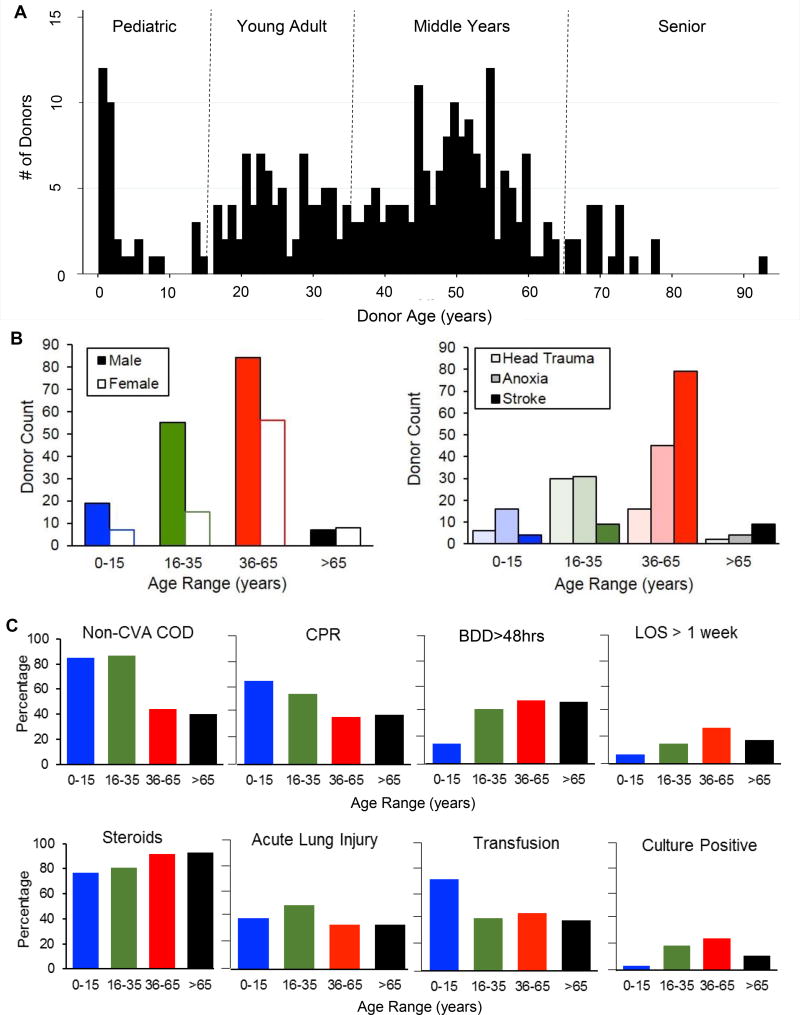
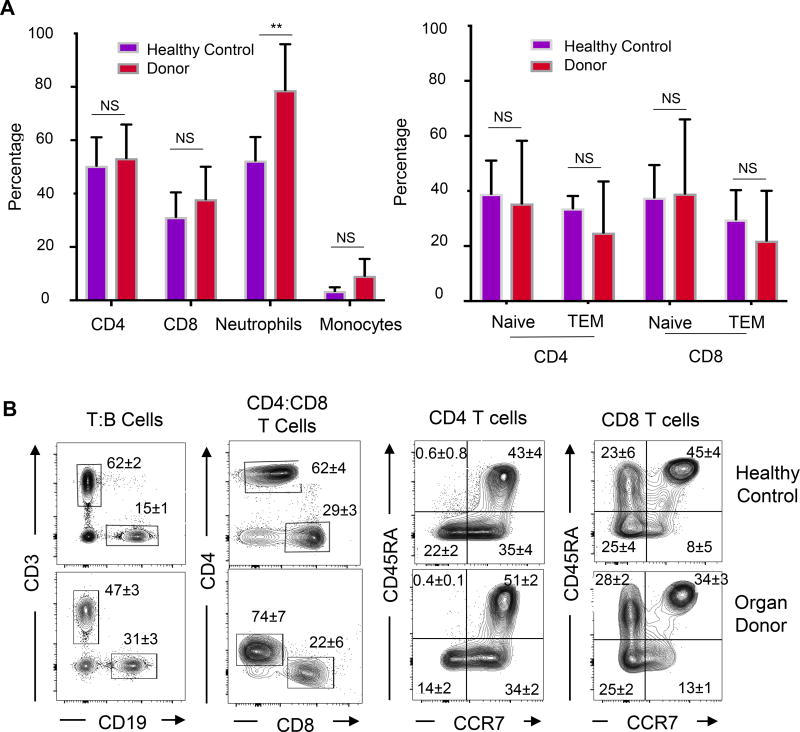
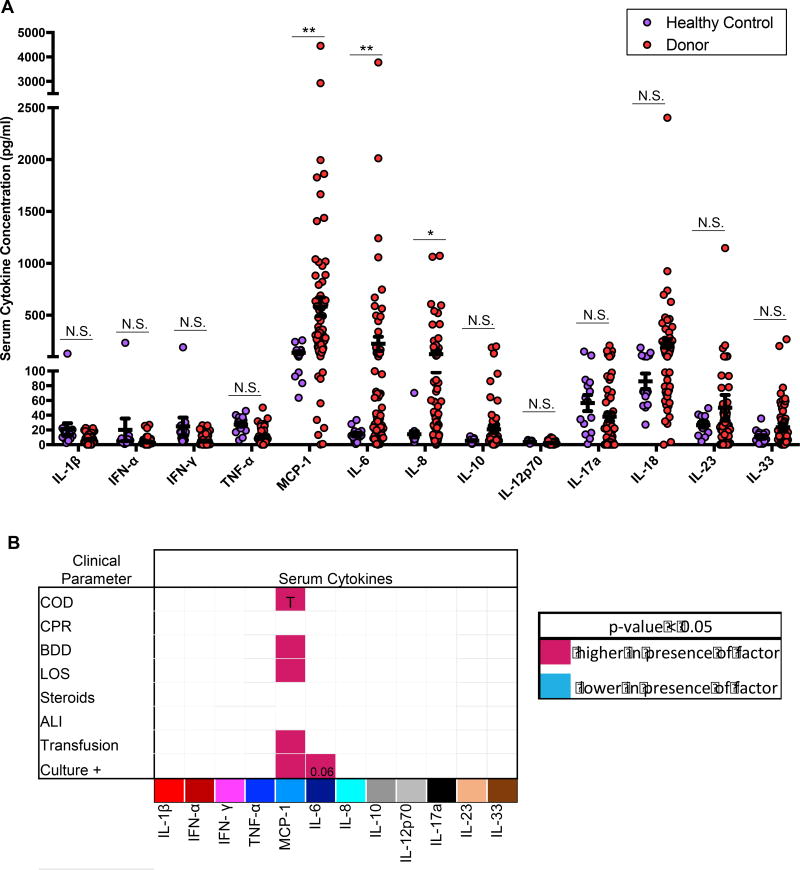
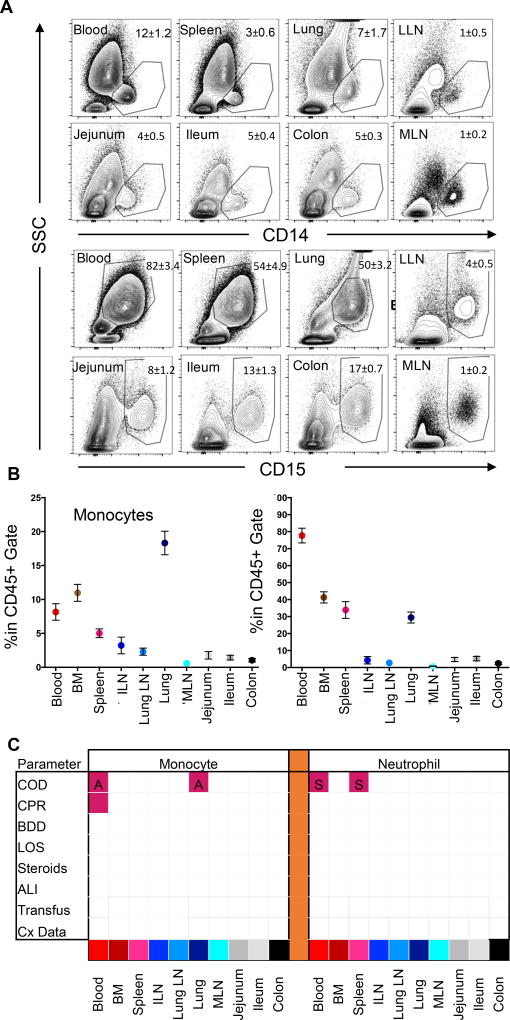
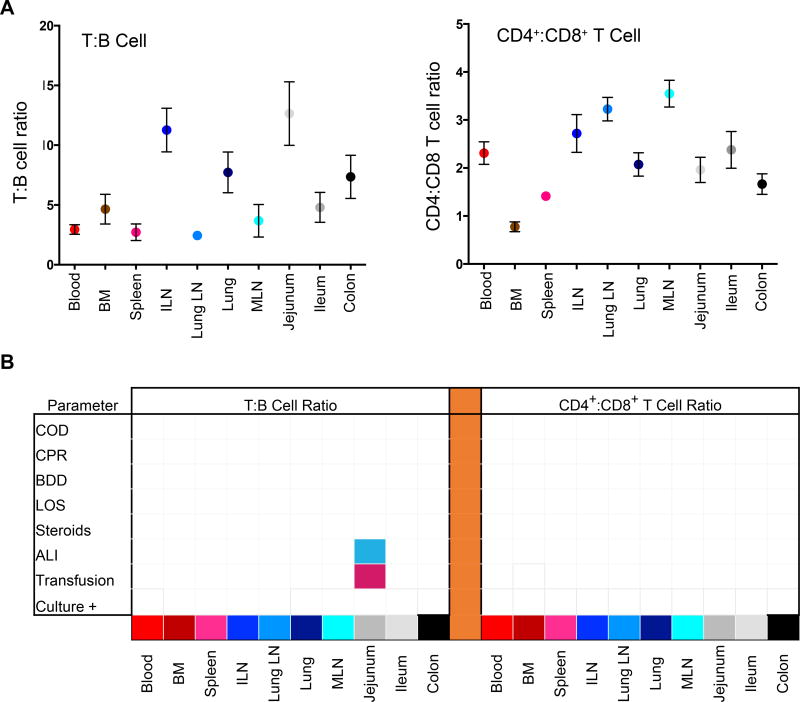
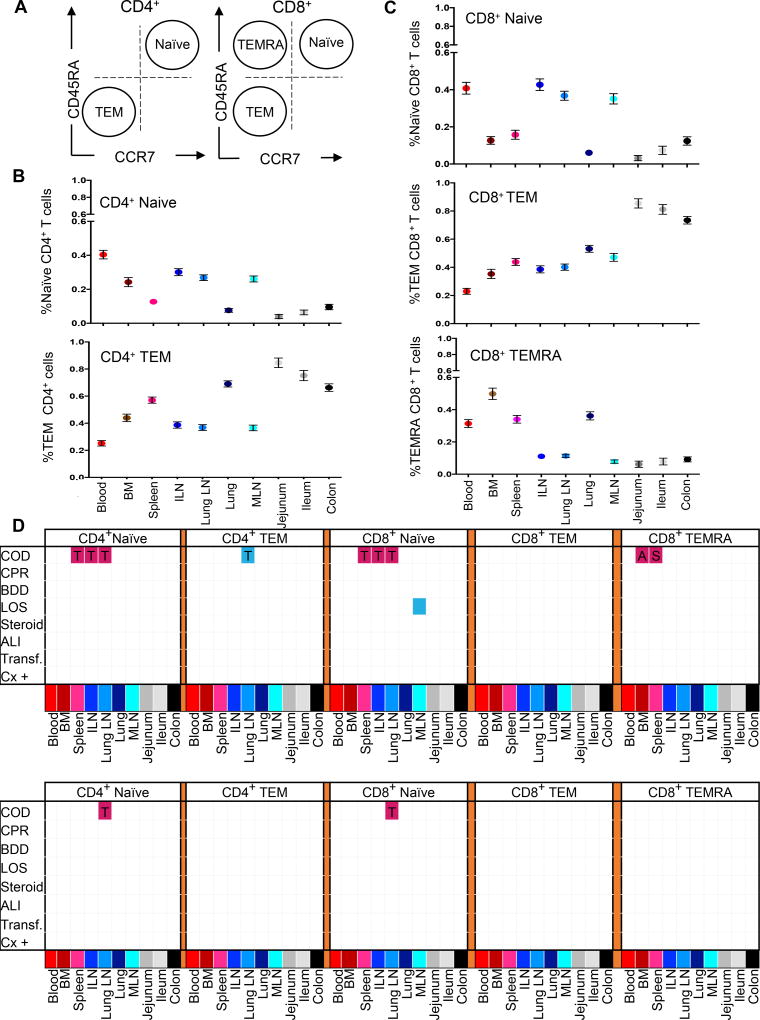
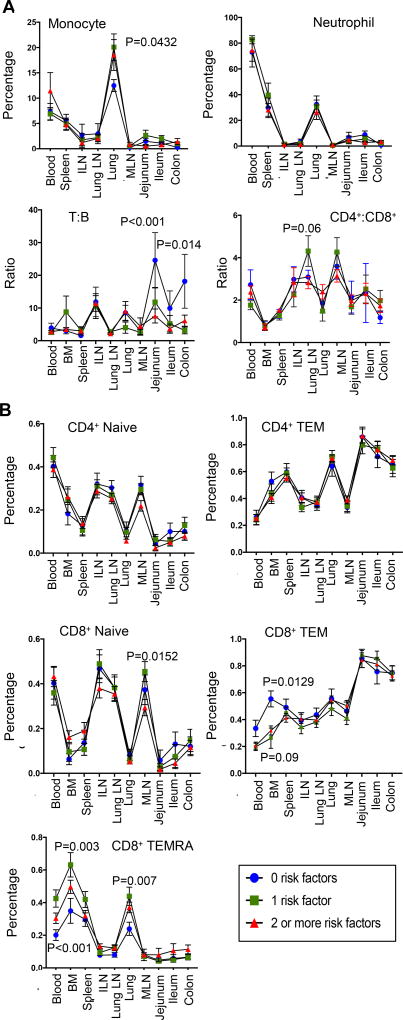
Organ donors are sources of physiologically healthy organs and tissues for life-saving transplantation, and have been recently used for human immunology studies which are typically confined to the sampling of peripheral blood. Donors comprise a diverse population with different causes of death and clinical outcomes during hospitalization, and the effects of such variations on immune parameters in blood and tissues are not known. We present here a coordinate analysis of innate and adaptive immune components in blood, lymphoid (bone marrow, spleen, lymph nodes), and mucosal (lungs, intestines) sites from a population of brain-dead organ donors (2 months-93 years; n = 291) across eight clinical parameters. Overall, the blood of donors exhibited similar monocyte and lymphocyte content and low serum levels of pro-inflammatory cytokines as healthy controls; however, donor blood had increased neutrophils and serum levels of IL-8, IL-6, and MCP-1 which varied with cause of death. In tissues, the frequency and composition of monocytes, neutrophils, B lymphocytes and T cell subsets in lymphoid or mucosal sites did not vary with clinical state, and was similar in donors independent of the extent of clinical complications. Our results reveal that organ donors maintain tissue homeostasis, and are a valuable resource for fundamental studies in human immunology.
Keywords: cellular biology; donors and donation: deceased; immune regulation; immunobiology; lymphocyte biology; monitoring: immune; organ procurement; organ procurement and allocation; translational research/science.
© 2017 The American Society of Transplantation and the American Society of Transplant Surgeons.
Conflict of interest statement
The authors of this manuscript have no conflicts of interest to disclose as described by the
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
