

Severity of Pneumonia in Under 5-Year-Old Children from Developing Countries: A Multicenter, Prospective, Observational Study
- PMID: 28719310
- PMCID: PMC5508893
- DOI: 10.4269/ajtmh.16-0733
Severity of Pneumonia in Under 5-Year-Old Children from Developing Countries: A Multicenter, Prospective, Observational Study
Abstract
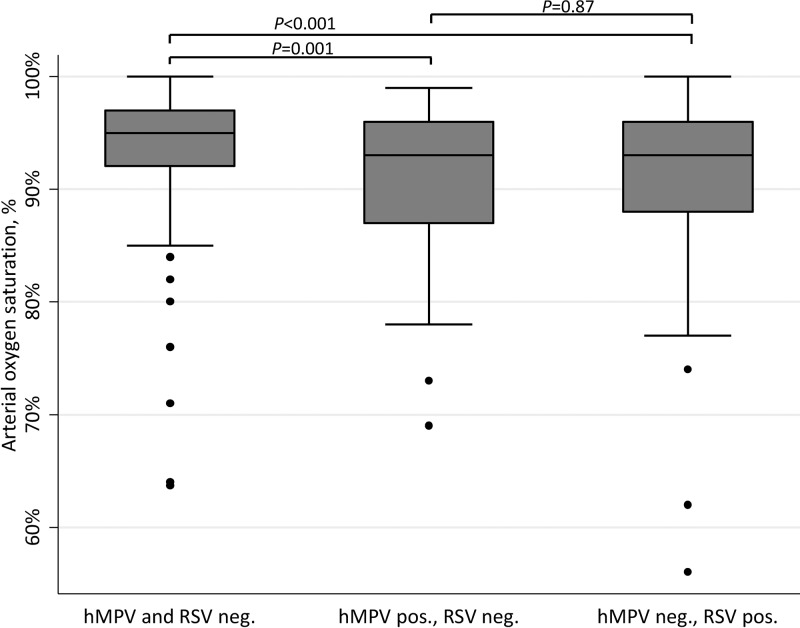
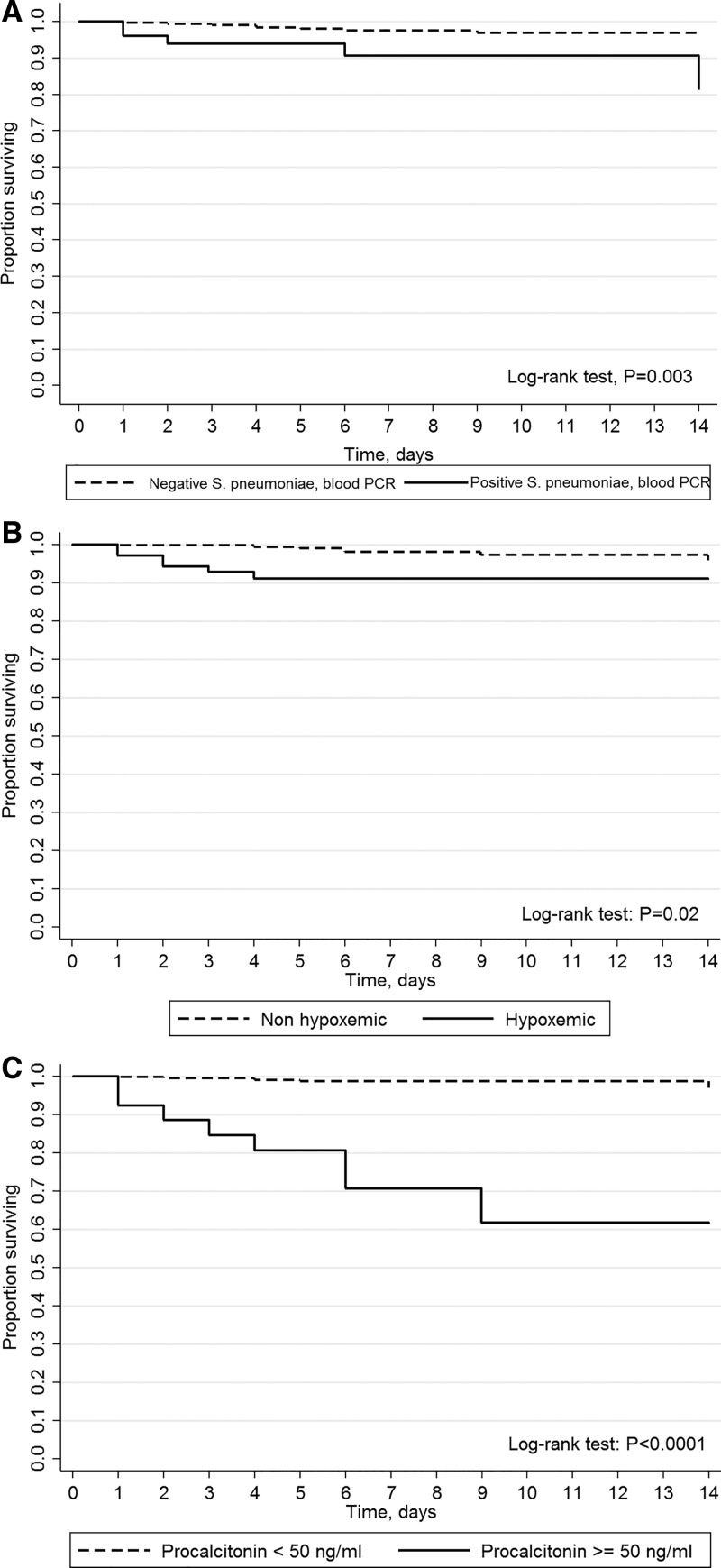
Pneumonia is the leading cause of death in children. The objectives were to evaluate the microbiological agents linked with hypoxemia in hospitalized children with pneumonia from developing countries, to identify predictors of hypoxemia, and to characterize factors associated with in-hospital mortality. A multicenter, observational study was conducted in five hospitals, from India (Lucknow, Vadu), Madagascar (Antananarivo), Mali (Bamako), and Paraguay (San Lorenzo). Children aged 2-60 months with radiologically confirmed pneumonia were enrolled prospectively. Respiratory and whole blood specimens were collected, identifying viruses and bacteria by real-time multiplex polymerase chain reaction (PCR). Microbiological agents linked with hypoxemia at admission (oxygen saturation < 90%) were analyzed by multivariate logistic regression, and factors associated with 14-day in-hospital mortality were assessed by bivariate Cox regression. Overall, 405 pneumonia cases (3,338 hospitalization days) were analyzed; 13 patients died within 14 days of hospitalization. Hypoxemia prevalence was 17.3%. Detection of human metapneumovirus (hMPV) and respiratory syncytial virus (RSV) in respiratory samples was independently associated with increased risk of hypoxemia (adjusted odds ratio [aOR] = 2.4, 95% confidence interval [95% CI] = 1.0-5.8 and aOR = 2.5, 95% CI = 1.1-5.3, respectively). Lower chest indrawing and cyanosis were predictive of hypoxemia (positive likelihood ratios = 2.3 and 2.4, respectively). Predictors of death were Streptococcus pneumoniae detection by blood PCR (crude hazard ratio [cHR] = 4.6, 95% CI = 1.5-14.0), procalcitonin ≥ 50 ng/mL (cHR = 22.4, 95% CI = 7.3-68.5) and hypoxemia (cHR = 4.8, 95% CI = 1.6-14.4). These findings were consistent on bivariate analysis. hMPV and RSV in respiratory samples were linked with hypoxemia, and S. pneumoniae in blood was associated with increased risk of death among hospitalized children with pneumonia in developing countries.
Figures
Similar articles
-
Etiology and Factors Associated with Pneumonia in Children under 5 Years of Age in Mali: A Prospective Case-Control Study.PLoS One. 2015 Dec 22;10(12):e0145447. doi: 10.1371/journal.pone.0145447. eCollection 2015. PLoS One. 2015. PMID: 26696249 Free PMC article.
-
Microorganisms Associated With Pneumonia in Children <5 Years of Age in Developing and Emerging Countries: The GABRIEL Pneumonia Multicenter, Prospective, Case-Control Study.Clin Infect Dis. 2017 Aug 15;65(4):604-612. doi: 10.1093/cid/cix378. Clin Infect Dis. 2017. PMID: 28605562 Free PMC article.
-
Viral and Atypical Bacterial Detection in Young Nepalese Children Hospitalized with Severe Pneumonia.Microbiol Spectr. 2021 Oct 31;9(2):e0055121. doi: 10.1128/Spectrum.00551-21. Epub 2021 Oct 27. Microbiol Spectr. 2021. PMID: 34704788 Free PMC article.
-
Multicenter case-control study protocol of pneumonia etiology in children: Global Approach to Biological Research, Infectious diseases and Epidemics in Low-income countries (GABRIEL network).BMC Infect Dis. 2014 Dec 10;14:635. doi: 10.1186/s12879-014-0635-8. BMC Infect Dis. 2014. PMID: 25927410 Free PMC article.
-
A preliminary study of pneumonia etiology among hospitalized children in Kenya.Clin Infect Dis. 2012 Apr;54 Suppl 2(Suppl 2):S190-9. doi: 10.1093/cid/cir1071. Clin Infect Dis. 2012. PMID: 22403235 Free PMC article.
Cited by
-
Burden of Influenza in Less Than 5-Year-Old Children Admitted to Hospital with Pneumonia in Developing and Emerging Countries: A Descriptive, Multicenter Study.Am J Trop Med Hyg. 2018 Jun;98(6):1805-1810. doi: 10.4269/ajtmh.17-0494. Epub 2018 Apr 12. Am J Trop Med Hyg. 2018. PMID: 29663903 Free PMC article.
-
Treatment of lung diseases via nanoparticles and nanorobots: Are these viable alternatives to overcome current treatments?Mater Today Bio. 2025 Feb 26;31:101616. doi: 10.1016/j.mtbio.2025.101616. eCollection 2025 Apr. Mater Today Bio. 2025. PMID: 40124344 Free PMC article. Review.
-
What are the risk factors for death among children with pneumonia in low- and middle-income countries? A systematic review.J Glob Health. 2023 Feb 24;13:05003. doi: 10.7189/jogh.13.05003. J Glob Health. 2023. PMID: 36825608 Free PMC article.
-
Feasibility and acceptability of the paediatric pulse oximeter in integrated management of neonatal and childhood illnesses (IMNCI) services by public health facilities: A qualitative study in rural Western India.J Glob Health. 2023 Sep 15;13:04105. doi: 10.7189/jogh.13.04105. J Glob Health. 2023. PMID: 37712148 Free PMC article.
-
The protective effect of Qingfei Huatan decoction on pulmonary function and its influence on the immunological function in children with severe pneumonia.Am J Transl Res. 2021 Aug 15;13(8):9404-9412. eCollection 2021. Am J Transl Res. 2021. PMID: 34540059 Free PMC article.
References
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, Cousens S, Mathers C, Black RE, 2015. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet 385: 430–440. - PubMed
-
- Subhi R, Adamson M, Campbell H, Weber M, Smith K, Duke T, Hypoxaemia in Developing Countries Study Group , 2009. The prevalence of hypoxaemia among ill children in developing countries: a systematic review. Lancet Infect Dis 9: 219–227. - PubMed
-
- Floyd J, Wu L, Hay Burgess D, Izadnegahdar R, Mukanga D, Ghani AC, 2015. Evaluating the impact of pulse oximetry on childhood pneumonia mortality in resource-poor settings. Nature 528: S53–S59. - PubMed
-
- Ginsburg AS, Cleve WCV, Thompson MIW, English M, 2012. Oxygen and pulse oximetry in childhood pneumonia: a survey of healthcare providers in resource-limited settings. J Trop Pediatr 58: 389–393. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
