

Serologic Responses in Childhood Pulmonary Tuberculosis
- PMID: 28719497
- PMCID: PMC6261442
- DOI: 10.1097/INF.0000000000001683
Serologic Responses in Childhood Pulmonary Tuberculosis
Abstract
Background: Identification of the Mycobacterium tuberculosis immunoproteome and antigens associated with serologic responses in adults has renewed interest in developing a serologic test for childhood tuberculosis (TB). We investigated IgG antibody responses against M. tuberculosis antigens in children with well-characterized TB.
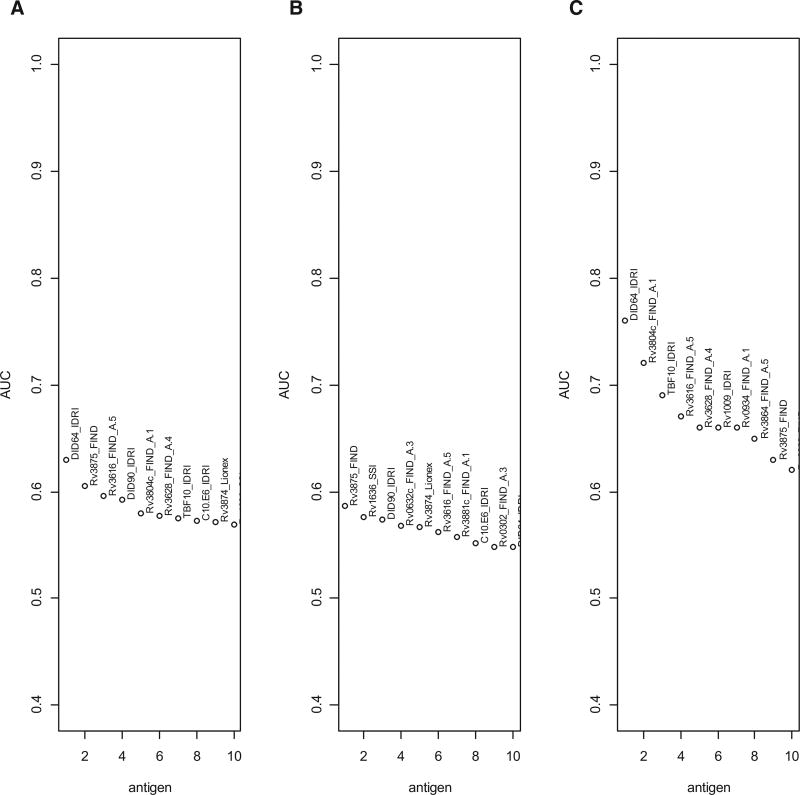
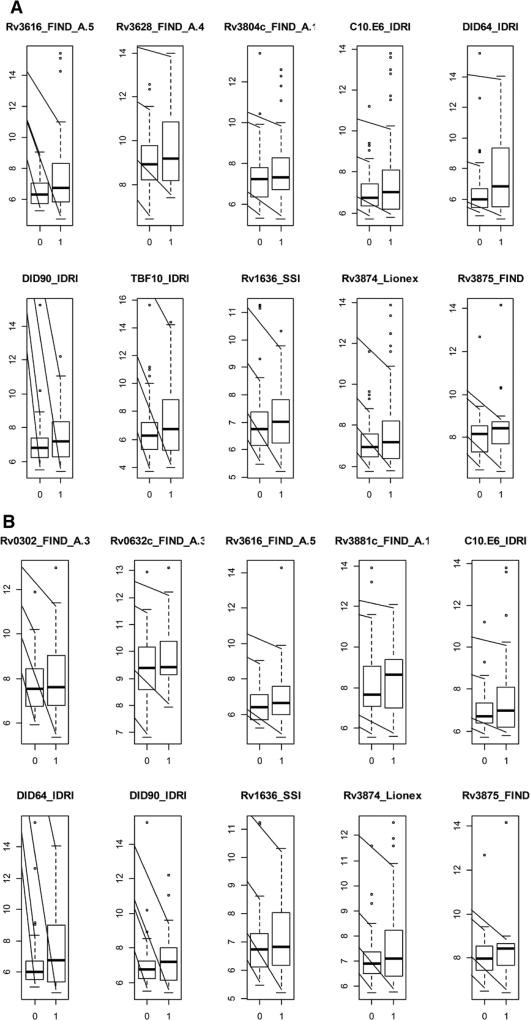
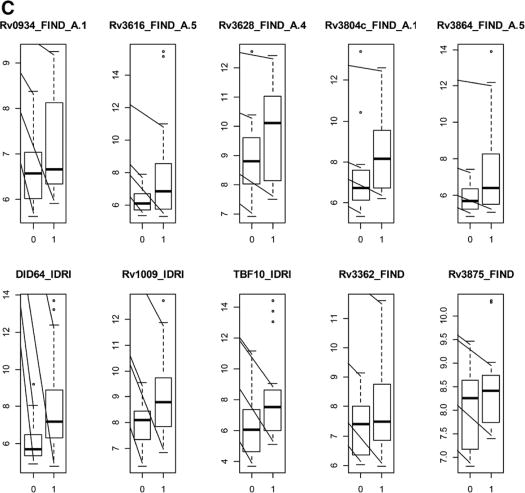
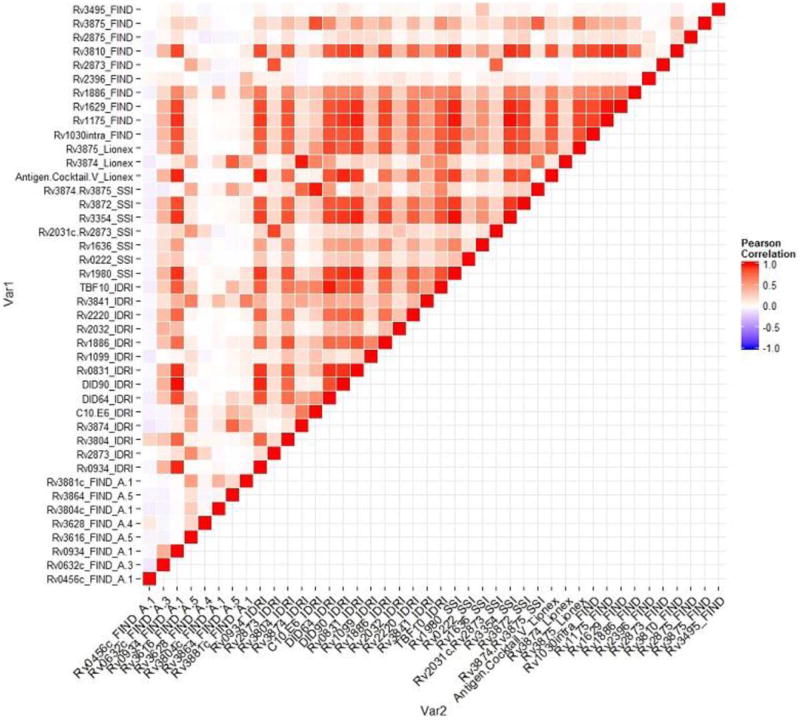
Methods: We studied archived sera obtained from hospitalized children with suspected pulmonary TB, and classified as having confirmed TB (culture-confirmed), unlikely TB (clinical improvement without TB treatment), or unconfirmed TB (all others). A multiplexed bead-based assay for IgG antibodies against 119 M. tuberculosis antigens was developed, validated and used to test sera. The area under the curves (AUCs) of the empiric receiver-operator characteristic curves were generated as measures of predictive ability. A cross-validated generalized linear model was used to select the most predictive combinations of antigens.
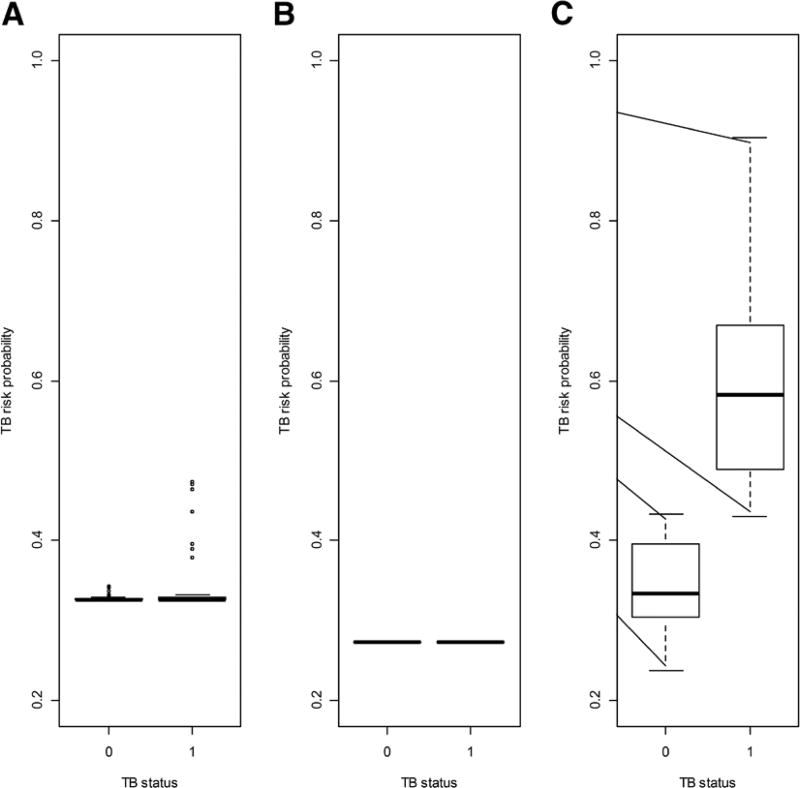
Results: For the confirmed TB versus unlikely TB comparison, the maximal single antigen AUC was 0.63, corresponding to sensitivity 0.60 and specificity 0.60. Older (age: 60+ months old) children's responses were better predictive of TB status than younger (age: 12-59 months old) children's, with a maximal single antigen AUC of -0.76. For the confirmed TB versus unlikely TB groups, the most predictive combinations of antigens assigned TB risk probabilities of 0.33 and 0.33, respectively, when all ages were considered, and 0.57 (interquartile range: 0.48-0.64) and 0.35 (interquartile range: 0.32-0.40) when only older children were considered.
Conclusion: An antigen-based IgG test is unlikely to meet the performance characteristics required of a TB detection test applicable to all age groups.
Conflict of interest statement
The other authors have no conflicts of interest to disclose.
Figures
References
-
- Dodd PJ, Gardiner E, Coghlan R, et al. Burden of childhood tuberculosis in 22 high-burden countries: a mathematical modelling study. Lancet Glob Health. 2014;2:e453–e459. - PubMed
-
- Dye C, Watt CJ, Bleed DM, et al. Evolution of tuberculosis control and prospects for reducing tuberculosis incidence, prevalence, and deaths globally. JAMA. 2005;293:2767–2775. - PubMed
-
- Moore HA, Apolles P, de Villiers PJ, et al. Sputum induction for microbiological diagnosis of childhood pulmonary tuberculosis in a community setting. Int J Tuberc Lung Dis. 2011;15:1185–1190. i. - PubMed
-
- Zar HJ, Connell TG, Nicol M. Diagnosis of pulmonary tuberculosis in children: new advances. Expert Rev Anti Infect Ther. 2010;8:277–288. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
