

Prehospital immune responses and development of multiple organ dysfunction syndrome following traumatic injury: A prospective cohort study
- PMID: 28719602
- PMCID: PMC5515405
- DOI: 10.1371/journal.pmed.1002338
Prehospital immune responses and development of multiple organ dysfunction syndrome following traumatic injury: A prospective cohort study
Abstract
Background: Almost all studies that have investigated the immune response to trauma have analysed blood samples acquired post-hospital admission. Thus, we know little of the immune status of patients in the immediate postinjury phase and how this might influence patient outcomes. The objective of this study was therefore to comprehensively assess the ultra-early, within 1-hour, immune response to trauma and perform an exploratory analysis of its relationship with the development of multiple organ dysfunction syndrome (MODS).
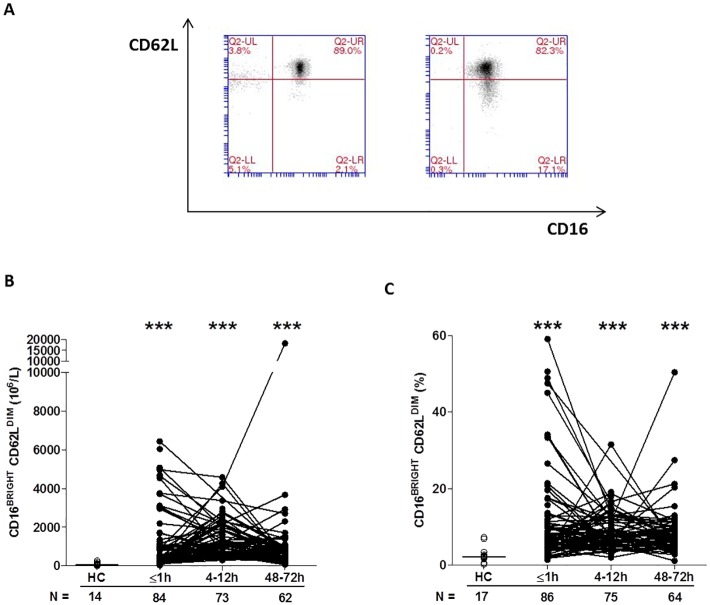
Methods and findings: The immune and inflammatory response to trauma was analysed in 89 adult trauma patients (mean age 41 years, range 18-90 years, 75 males) with a mean injury severity score (ISS) of 24 (range 9-66), from whom blood samples were acquired within 1 hour of injury (mean time to sample 42 minutes, range 17-60 minutes). Within minutes of trauma, a comprehensive leukocytosis, elevated serum pro- and anti-inflammatory cytokines, and evidence of innate cell activation that included neutrophil extracellular trap generation and elevated surface expression of toll-like receptor 2 and CD11b on monocytes and neutrophils, respectively, were observed. Features consistent with immune compromise were also detected, notably elevated numbers of immune suppressive CD16BRIGHT CD62LDIM neutrophils (82.07 x 106/l ± 18.94 control versus 1,092 x 106/l ± 165 trauma, p < 0.0005) and CD14+HLA-DRlow/- monocytes (34.96 x 106/l ± 4.48 control versus 95.72 x 106/l ± 8.0 trauma, p < 0.05) and reduced leukocyte cytokine secretion in response to lipopolysaccharide stimulation. Exploratory analysis via binary logistic regression found a potential association between absolute natural killer T (NKT) cell numbers and the subsequent development of MODS. Study limitations include the relatively small sample size and the absence of data relating to adaptive immune cell function.
Conclusions: Our study highlighted the dynamic and complex nature of the immune response to trauma, with immune alterations consistent with both activation and suppression evident within 1 hour of injury. The relationship of these changes, especially in NKT cell numbers, to patient outcomes such as MODS warrants further investigation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures






References
-
- Giannoudis PV. Current concepts of the inflammatory response after major trauma: an update. Injury. 2003; 34:397–404. - PubMed
-
- Hazeldine J, Hampson P, Lord JM. The diagnostic and prognostic value of systems biology research in major traumatic and thermal injury: a review. Burns and Trauma. 2016. doi: 10.1186/s41038-016-0059-3 - DOI - PMC - PubMed
-
- Hampson P, Dinsdale RJ, Wearn CM, Bamford AL, Bishop JR, Hazeldine J, et al. Neutrophil Dysfunction, Immature Granulocytes, and Cell-free DNA are Early Biomarkers of Sepsis in Burn-injured Patients: A Prospective Observational Cohort Study. Ann.Surg. 2016. doi: 10.1097/SLA.0000000000001807 - DOI - PubMed
-
- Liao Y, Liu P, Guo F, Zhang ZY, Zhang Z. Oxidative burst of circulating neutrophils following traumatic brain injury in human. PLoS ONE. 2013. 8: e68963 doi: 10.1371/journal.pone.0068963 - DOI - PMC - PubMed
-
- Li H, Itagaki K, Sandler N, Gallo D, Galenkamp A, Kaczmarek E, et al. Mitochondrial damage-associated molecular patterns from fractures suppress pulmonary immune responses via formyl peptide receptors 1 and 2. J.Trauma Acute.Care Surg. 2015;78: 272–279. doi: 10.1097/TA.0000000000000509 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
