

Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fibre density in diabetic neuropathy
- PMID: 28719619
- PMCID: PMC5515394
- DOI: 10.1371/journal.pone.0180175
Diagnostic utility of corneal confocal microscopy and intra-epidermal nerve fibre density in diabetic neuropathy
Abstract
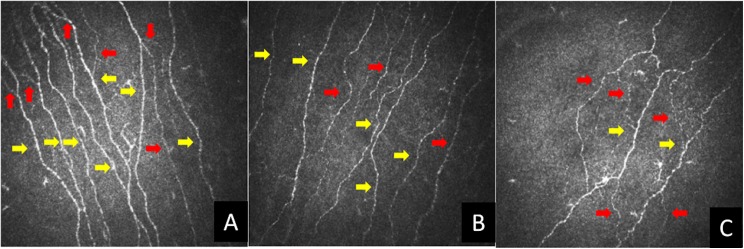
Objectives: Corneal confocal microscopy (CCM) is a rapid, non-invasive, reproducible technique that quantifies small nerve fibres. We have compared the diagnostic capability of CCM against a range of established measures of nerve damage in patients with diabetic neuropathy.
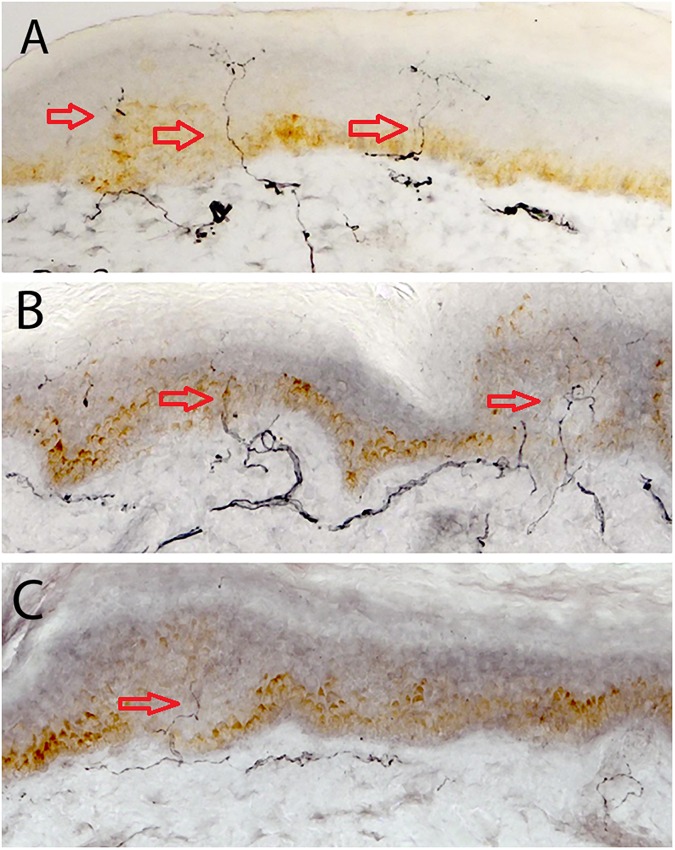
Methods: In this cross sectional study, thirty subjects with Type 1 diabetes without neuropathy (T1DM), thirty one T1DM subjects with neuropathy (DSPN) and twenty seven non-diabetic healthy control subjects underwent detailed assessment of neuropathic symptoms and neurologic deficits, quantitative sensory testing (QST), electrophysiology, skin biopsy and corneal confocal microscopy (CCM).
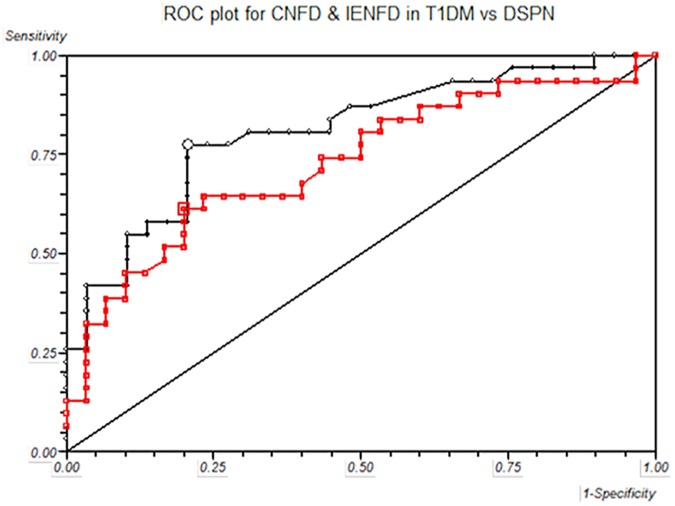
Results: Subjects with DSPN were older (C vs T1DM vs DSPN: 41.0±14.9 vs 38.8±12.5 vs 53.3±11.9, P = 0.0002), had a longer duration of diabetes (P<0.0001), lower eGFR (P = 0.006) and higher albumin-creatinine ratio (P = 0.03) with no significant difference for HbA1c, BMI, lipids and blood pressure. Patients with DSPN were representative of subjects with diabetic neuropathy with clinical signs and symptoms of neuropathy and greater neuropathy deficits quantified by QST, electrophysiology, intra-epidermal nerve fibre density and CCM. Corneal nerve fibre density (CNFD) (Spearman's Rho = 0.60 P<0.0001) and IENFD (Spearman's Rho = 0.56 P<0.0001) were comparable when correlated with peroneal nerve conduction velocity. For the diagnosis of diabetic neuropathy the sensitivity for CNFD was 0.77 and specificity was 0.79 with an area under the ROC curve of 0.81. IENFD had a diagnostic sensitivity of 0.61, specificity of 0.80 and area under the ROC curve of 0.73.
Conclusions: CCM is a valid accurate non-invasive method to identify small nerve fibre pathology and is able to diagnose DPN.
Conflict of interest statement
Figures
References
-
- Dyck PJ, Herrmann DN, Staff NP. Assessing decreased sensation and increased sensory phenomena in diabetic polyneuropathies. Diabetes. 2013;62(11):3677–86. Epub 2013/10/26. doi: 10.2337/db13-0352 . - DOI - PMC - PubMed
-
- Dyck PJ, Overland CJ, Low PA, Litchy WJ, Davies JL, O'Brien PC, et al. Signs and symptoms versus nerve conduction studies to diagnose diabetic sensorimotor polyneuropathy: Cl vs. NPhys trial. Muscle Nerve. 2010;42(2):157–64. Epub 2010/07/27. doi: 10.1002/mus.21661 ; PubMed Central PMCID: PMC2956592. - DOI - PMC - PubMed
-
- Dyck PJ, Argyros B, Russell JW, Gahnstrom LE, Nalepa S, Albers JW, et al. Multicenter trial of the proficiency of smart quantitative sensation tests. Muscle Nerve. 2014;49(5):645–53. Epub 2013/08/10. doi: 10.1002/mus.23982 . - DOI - PMC - PubMed
-
- Tesfaye S, Boulton AJ, Dyck PJ, Freeman R, Horowitz M, Kempler P, et al. Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care. 2010;33(10):2285–93. Epub 2010/09/30. doi: 10.2337/dc10-1303 ; PubMed Central PMCID: PMC2945176. - DOI - PMC - PubMed
-
- Sumner CJ, Sheth S, Griffin JW, Cornblath DR, Polydefkis M. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology. 2003;60(1):108–11. Epub 2003/01/15. . - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
