

Association of Changing Hospital Readmission Rates With Mortality Rates After Hospital Discharge
- PMID: 28719692
- PMCID: PMC5817448
- DOI: 10.1001/jama.2017.8444
Association of Changing Hospital Readmission Rates With Mortality Rates After Hospital Discharge
Abstract
Importance: The Affordable Care Act has led to US national reductions in hospital 30-day readmission rates for heart failure (HF), acute myocardial infarction (AMI), and pneumonia. Whether readmission reductions have had the unintended consequence of increasing mortality after hospitalization is unknown.
Objective: To examine the correlation of paired trends in hospital 30-day readmission rates and hospital 30-day mortality rates after discharge.
Design, setting, and participants: Retrospective study of Medicare fee-for-service beneficiaries aged 65 years or older hospitalized with HF, AMI, or pneumonia from January 1, 2008, through December 31, 2014.
Exposure: Thirty-day risk-adjusted readmission rate (RARR).
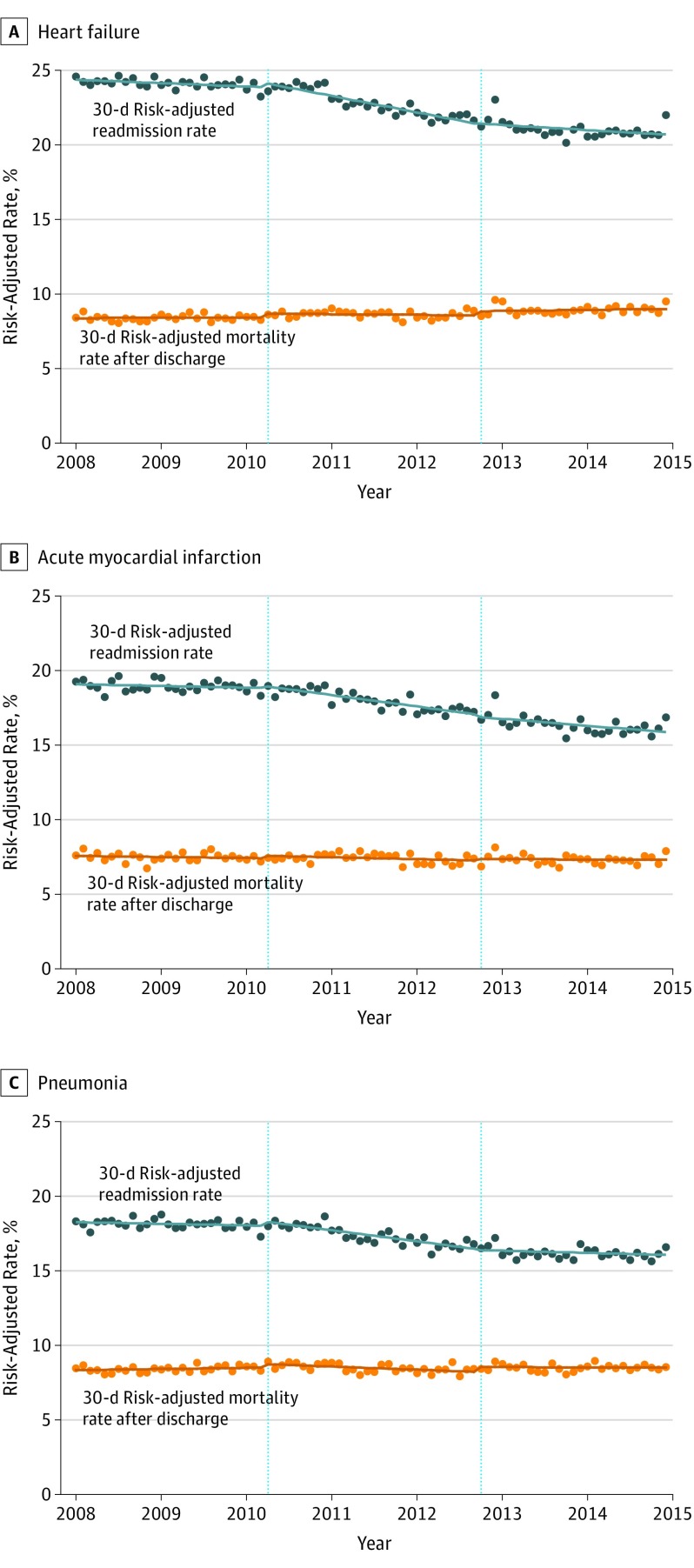
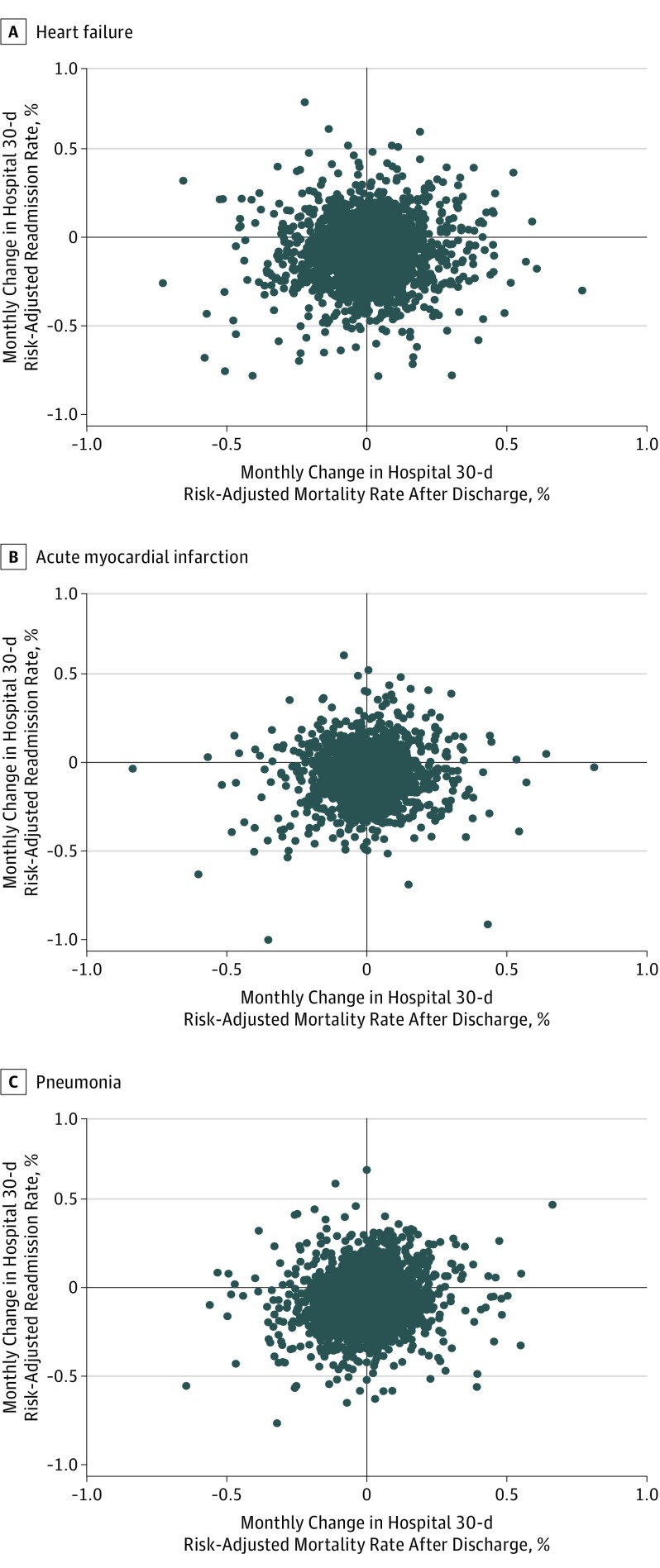
Main outcomes and measures: Thirty-day RARRs and 30-day risk-adjusted mortality rates (RAMRs) after discharge were calculated for each condition in each month at each hospital in 2008 through 2014. Monthly trends in each hospital's 30-day RARRs and 30-day RAMRs after discharge were examined for each condition. The weighted Pearson correlation coefficient was calculated for hospitals' paired monthly trends in 30-day RARRs and 30-day RAMRs after discharge for each condition.
Results: In 2008 through 2014, 2 962 554 hospitalizations for HF, 1 229 939 for AMI, and 2 544 530 for pneumonia were identified at 5016, 4772, and 5057 hospitals, respectively. In January 2008, mean hospital 30-day RARRs and 30-day RAMRs after discharge were 24.6% and 8.4% for HF, 19.3% and 7.6% for AMI, and 18.3% and 8.5% for pneumonia. Hospital 30-day RARRs declined in the aggregate across hospitals from 2008 through 2014; monthly changes in RARRs were -0.053% (95% CI, -0.055% to -0.051%) for HF, -0.044% (95% CI, -0.047% to -0.041%) for AMI, and -0.033% (95% CI, -0.035% to -0.031%) for pneumonia. In contrast, monthly aggregate changes across hospitals in hospital 30-day RAMRs after discharge varied by condition: HF, 0.008% (95% CI, 0.007% to 0.010%); AMI, -0.003% (95% CI, -0.005% to -0.001%); and pneumonia, 0.001% (95% CI, -0.001% to 0.003%). However, correlation coefficients in hospitals' paired monthly changes in 30-day RARRs and 30-day RAMRs after discharge were weakly positive: HF, 0.066 (95% CI, 0.036 to 0.096); AMI, 0.067 (95% CI, 0.027 to 0.106); and pneumonia, 0.108 (95% CI, 0.079 to 0.137). Findings were similar in secondary analyses, including with alternate definitions of hospital mortality.
Conclusions and relevance: Among Medicare fee-for-service beneficiaries hospitalized for heart failure, acute myocardial infarction, or pneumonia, reductions in hospital 30-day readmission rates were weakly but significantly correlated with reductions in hospital 30-day mortality rates after discharge. These findings do not support increasing postdischarge mortality related to reducing hospital readmissions.
Conflict of interest statement
Figures
Comment in
-
Readmissions Have Declined, and Mortality Has Not Increased: The Importance of Evaluating Unintended Consequences.JAMA. 2017 Jul 18;318(3):243-244. doi: 10.1001/jama.2017.8705. JAMA. 2017. PMID: 28719675 No abstract available.
-
Consequences of Reductions in Hospital Readmissions.JAMA. 2017 Nov 21;318(19):1933-1934. doi: 10.1001/jama.2017.14779. JAMA. 2017. PMID: 29164247 No abstract available.
References
-
- Zuckerman RB, Sheingold SH, Orav EJ, Ruhter J, Epstein AM. Readmissions, observation, and the Hospital Readmissions Reduction Program. N Engl J Med. 2016;374(16):1543-1551. - PubMed
-
- Naylor MD, Kurtzman ET, Grabowski DC, Harrington C, McClellan M, Reinhard SC. Unintended consequences of steps to cut readmissions and reform payment may threaten care of vulnerable older adults. Health Aff (Millwood). 2012;31(7):1623-1632. - PubMed
-
- Himmelstein D, Woolhandler S Quality improvement: ‘become good at cheating and you never need to become good at anything else.’ Health Affairs Blog August 27, 2015. http://healthaffairs.org/blog/2015/08/27/quality-improvement-become-good.... Accessed November 12, 2016.
-
- Carlson J. Faulty gauge? Readmissions are down, but observational-status patients are up—and that could skew Medicare numbers. Modern Healthcare June 8, 2013. http://www.modernhealthcare.com/article/20130608/magazine/306089991. Accessed November 12, 2016.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
