

A prolonged, community-wide cholera outbreak associated with drinking water contaminated by sewage in Kasese District, western Uganda
- PMID: 28720083
- PMCID: PMC5516304
- DOI: 10.1186/s12889-017-4589-9
A prolonged, community-wide cholera outbreak associated with drinking water contaminated by sewage in Kasese District, western Uganda
Erratum in
-
Erratum to: BMC Public Health, Vol. 18.BMC Public Health. 2017 Sep 22;17(1):736. doi: 10.1186/s12889-017-4709-6. BMC Public Health. 2017. PMID: 28938882 Free PMC article. No abstract available.
Abstract
Background: In May 2015, a cholera outbreak that had lasted 3 months and infected over 100 people was reported in Kasese District, Uganda, where multiple cholera outbreaks had occurred previously. We conducted an investigation to identify the mode of transmission to guide control measures.
Methods: We defined a suspected case as onset of acute watery diarrhoea from 1 February 2015 onwards in a Kasese resident. A confirmed case was a suspected case with Vibrio cholerae O1 El Tor, serotype Inaba cultured from a stool sample. We reviewed medical records to find cases. We conducted a case-control study to compare exposures among confirmed case-persons and asymptomatic controls, matched by village and age-group. We conducted environmental assessments. We tested water samples from the most affected area for total coliforms using the Most Probable Number (MPN) method.
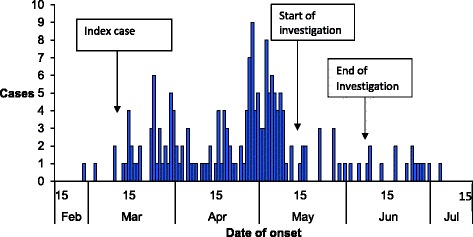
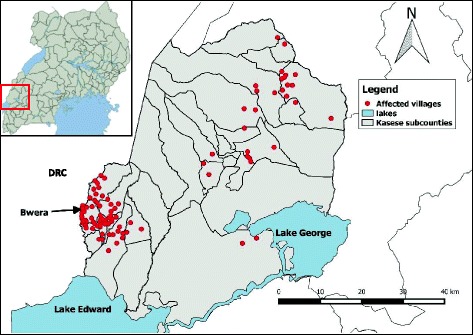
Results: We identified 183 suspected cases including 61 confirmed cases of Vibrio cholerae 01; serotype Inaba, with onset between February and July 2015. 2 case-persons died of cholera. The outbreak occurred in 80 villages and affected all age groups; the highest attack rate occurred in the 5-14 year age group (4.1/10,000). The outbreak started in Bwera Sub-County bordering the Democratic Republic of Congo and spread eastward through sustained community transmission. The first case-persons were involved in cross-border trading. The case-control study, which involved 49 confirmed cases and 201 controls, showed that 94% (46/49) of case-persons compared with 79% (160/201) of control-persons drank water without boiling or treatment (ORM-H=4.8, 95% CI: 1.3-18). Water collected from the two main sources, i.e., public pipes (consumed by 39% of case-persons and 38% of control-persons) or streams (consumed by 29% of case-persons and 24% control-persons) had high coliform counts, a marker of faecal contamination. Environmental assessment revealed evidence of open defecation along the streams. No food items were significantly associated with illness.
Conclusions: This prolonged, community-wide cholera outbreak was associated with drinking water contaminated by faecal matter and cross-border trading. We recommended rigorous disposal of patients' faeces, chlorination of piped water, and boiling or treatment of drinking water. The outbreak stopped 6 weeks after these recommendations were implemented.
Keywords: Case-control studies; Cholera; Outbreak; Uganda.
Conflict of interest statement
Ethics approval and consent to participate
This investigation was in response to a public health emergency and was therefore determined to be non-research. The investigation was authorized by MoH. Verbal informed consent in the local language was sought from respondents or care-takers of diseased children. They were informed that their participation was voluntary and their refusal would not result in any negative consequences. Ill participants were referred for free treatment at Government health facilities. To protect the confidentiality of the respondents, each was assigned a unique identifier which was used instead of their names.
Consent for publication
Not applicable.
Competing interests
We declare that there are no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- World Health Organisation cholera fact sheet [http://www.who.int/mediacentre/factsheets/fs107/en/].
-
- Ley B, Khatib AM, Thriemer K, von Seidlein L, Deen J, Mukhopadyay A, Chang N-Y, Hashim R, Schmied W, Busch CJL, et al. Evaluation of a rapid dipstick (crystal VC) for the diagnosis of cholera in Zanzibar and a comparison with previous studies. PLoS One. 2012;7(5) doi: 10.1371/journal.pone.0036930. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
