

Cardiovascular magnetic resonance in an adult human population: serial observations from the multi-ethnic study of atherosclerosis
- PMID: 28720123
- PMCID: PMC5514469
- DOI: 10.1186/s12968-017-0367-1
Cardiovascular magnetic resonance in an adult human population: serial observations from the multi-ethnic study of atherosclerosis
Abstract
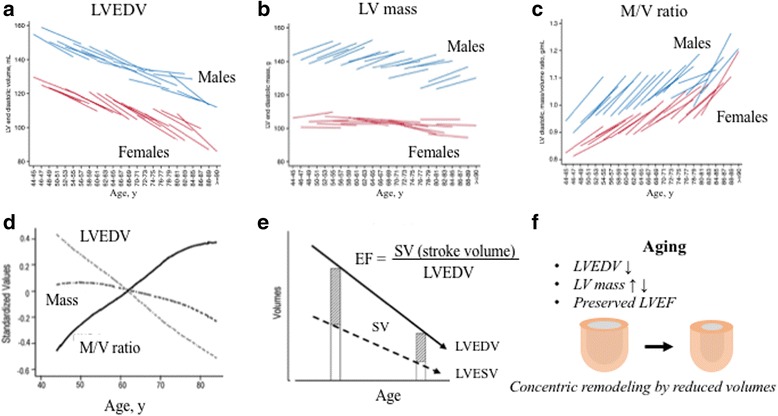
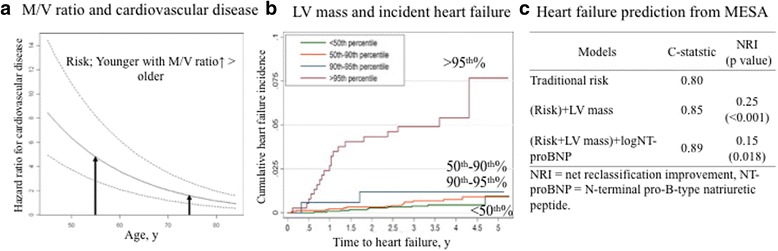
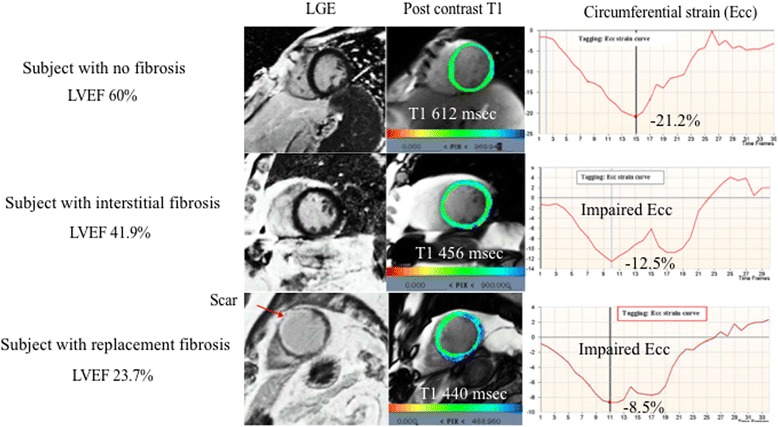
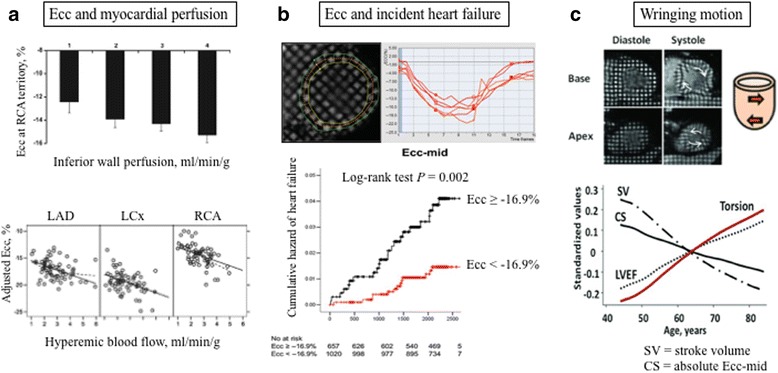
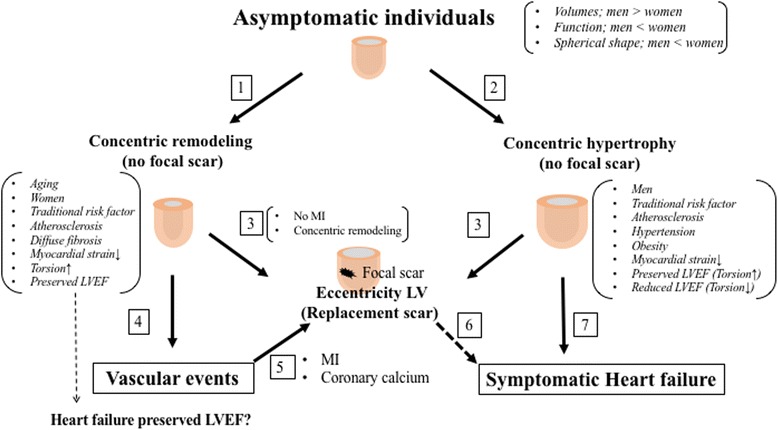
The Multi-Ethnic Study of Atherosclerosis (MESA) is the first large-scale multi-ethnic population study in the U.S. to use advanced cardiovascular magnetic resonance (CMR) imaging. MESA participants were free of cardiovascular disease at baseline between 2000 and 2002, and were followed up between 2009 and 2011 with repeated CMR examinations as part of MESA. CMR allows the clinician to visualize and accurately quantify volume and dimensions of all four cardiac chambers; measure systolic and diastolic ventricular function; assess myocardial fibrosis; assess vessel lumen size, vessel wall morphology, and vessel stiffness. CMR has a number of advantages over other imaging modalities such as echocardiography, computed tomography, and invasive angiography, and has been proposed as a diagnostic strategy for high-risk populations. MESA has been extensively evaluating CMR imaging biomarkers, as markers of subclinical disease, in the last 15 years for low-risk populations. On a more practical level, some of the imaging biomarkers developed and studied are translatable to at-risk populations. In this review, we discuss the progression of subclinical cardiovascular disease and the mechanisms responsible for the transition to symptomatic clinical outcomes based on our findings from MESA.
Keywords: Ageing; Cardiovascular disease; Fibrosis; Heart failure; Torsion.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors declare their consent for publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Late effects of pediatric hematopoietic stem cell transplantation on left ventricular function, aortic stiffness and myocardial tissue characteristics.J Cardiovasc Magn Reson. 2019 Jan 17;21(1):6. doi: 10.1186/s12968-018-0513-4. J Cardiovasc Magn Reson. 2019. PMID: 30651110 Free PMC article.
-
Natural History of Myocardial Function in an Adult Human Population: Serial Longitudinal Observations From MESA.JACC Cardiovasc Imaging. 2016 Oct;9(10):1164-1173. doi: 10.1016/j.jcmg.2016.01.038. Epub 2016 Sep 14. JACC Cardiovasc Imaging. 2016. PMID: 27639760
-
Magnetic Resonance Characterization of Cardiac Adaptation and Myocardial Fibrosis in Pulmonary Hypertension Secondary to Systemic-To-Pulmonary Shunt.Circ Cardiovasc Imaging. 2016 Sep;9(9):e004566. doi: 10.1161/CIRCIMAGING.116.004566. Circ Cardiovasc Imaging. 2016. PMID: 27601365
-
Clinical utility of cardiovascular magnetic resonance in hypertrophic cardiomyopathy.J Cardiovasc Magn Reson. 2012 Feb 1;14(1):13. doi: 10.1186/1532-429X-14-13. J Cardiovasc Magn Reson. 2012. PMID: 22296938 Free PMC article. Review.
-
CMR publications from China of the last more than 30 years.Int J Cardiovasc Imaging. 2020 Sep;36(9):1737-1747. doi: 10.1007/s10554-020-01873-x. Epub 2020 May 11. Int J Cardiovasc Imaging. 2020. PMID: 32394180
Cited by
-
Genetics of Cardiac Aging Implicate Organ-Specific Variation.medRxiv [Preprint]. 2024 Aug 6:2024.08.02.24310874. doi: 10.1101/2024.08.02.24310874. medRxiv. 2024. PMID: 39148824 Free PMC article. Preprint.
-
Relationship Between Vascular Aging and Left Ventricular Concentric Geometry in Community-Dwelling Elderly: The Northern Shanghai Study.Clin Interv Aging. 2020 Jun 4;15:853-863. doi: 10.2147/CIA.S248816. eCollection 2020. Clin Interv Aging. 2020. PMID: 32606625 Free PMC article.
-
Myocardial injury after major non-cardiac surgery evaluated with advanced cardiac imaging: a pilot study.BMC Cardiovasc Disord. 2023 Feb 10;23(1):78. doi: 10.1186/s12872-023-03065-6. BMC Cardiovasc Disord. 2023. PMID: 36765313 Free PMC article.
-
Cardiac MRI for Patients with Increased Cardiometabolic Risk.Radiol Cardiothorac Imaging. 2021 Apr 1;3(2):e200575. doi: 10.1148/ryct.2021200575. eCollection 2021 Apr. Radiol Cardiothorac Imaging. 2021. PMID: 33969314 Free PMC article.
-
Characterization of subclinical diastolic dysfunction by cardiac magnetic resonance feature-tracking in adult survivors of non-Hodgkin lymphoma treated with anthracyclines.BMC Cardiovasc Disord. 2021 Apr 12;21(1):170. doi: 10.1186/s12872-021-01996-6. BMC Cardiovasc Disord. 2021. PMID: 33845778 Free PMC article.
References
-
- Kawel N, Turkbey EB, Carr JJ, Eng J, Gomes AS, Hundley WG, et al. Normal left ventricular myocardial thickness for middle-aged and older subjects with steady-state free precession cardiac magnetic resonance: the multi-ethnic study of atherosclerosis. Circ Cardiovasc Imaging. 2012;5:500–508. doi: 10.1161/CIRCIMAGING.112.973560. - DOI - PMC - PubMed
-
- Heckbert SR, Post W, Pearson GD, Arnett DK, Gomes AS, Jerosch-Herold M, et al. Traditional cardiovascular risk factors in relation to left ventricular mass, volume, and systolic function by cardiac magnetic resonance imaging: the multiethnic study of atherosclerosis. J Am Coll Cardiol. 2006;48:2285–2292. doi: 10.1016/j.jacc.2006.03.072. - DOI - PMC - PubMed
-
- Cheng S, Fernandes VR, Bluemke DA, McClelland RL, Kronmal RA, Lima JA. Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: the multi-ethnic study of atherosclerosis. Circ Cardiovasc Imaging. 2009;2:191–198. doi: 10.1161/CIRCIMAGING.108.819938. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
