

FMR1 CGG repeat expansion mutation detection and linked haplotype analysis for reliable and accurate preimplantation genetic diagnosis of fragile X syndrome
- PMID: 28720156
- PMCID: PMC5733830
- DOI: 10.1017/erm.2017.10
FMR1 CGG repeat expansion mutation detection and linked haplotype analysis for reliable and accurate preimplantation genetic diagnosis of fragile X syndrome
Abstract
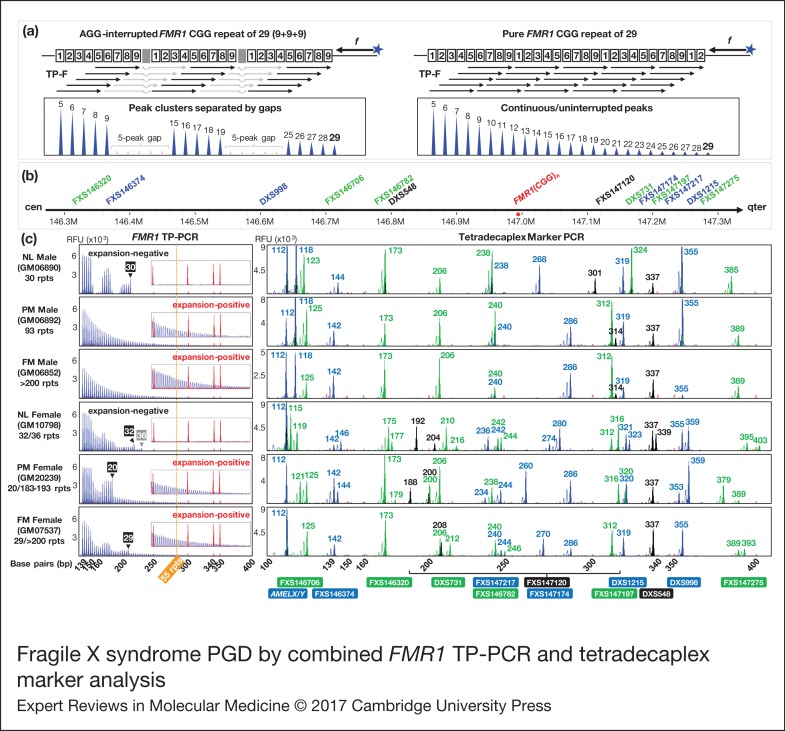
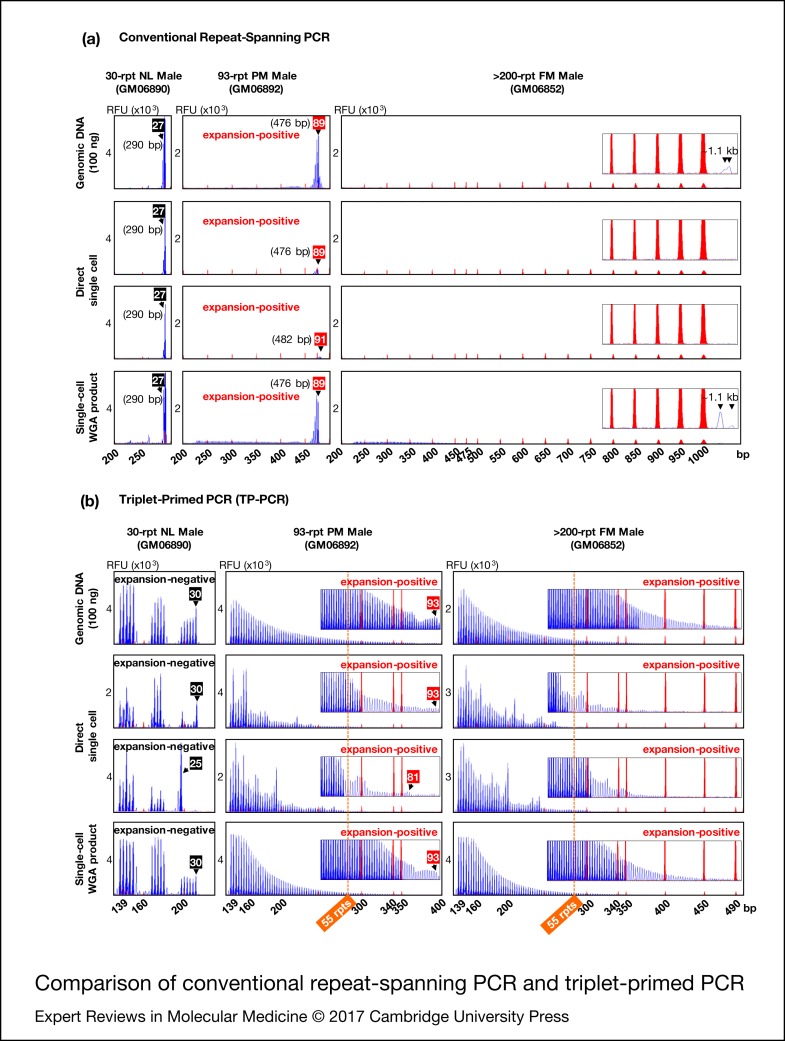
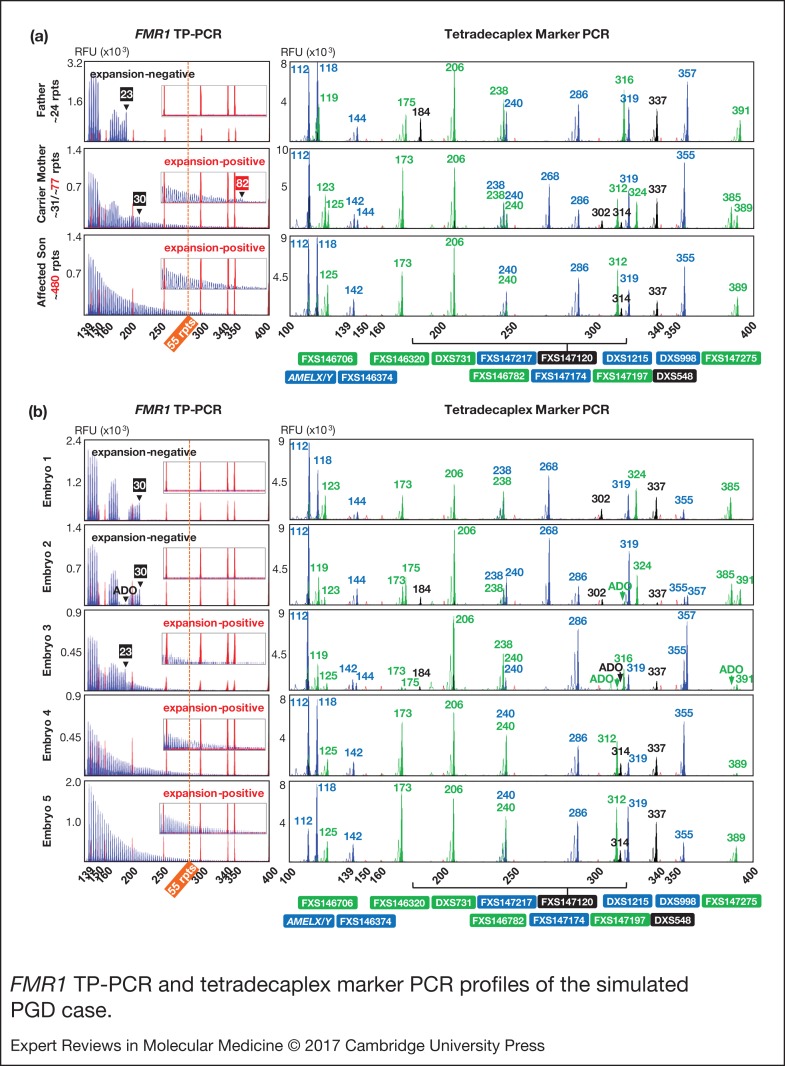
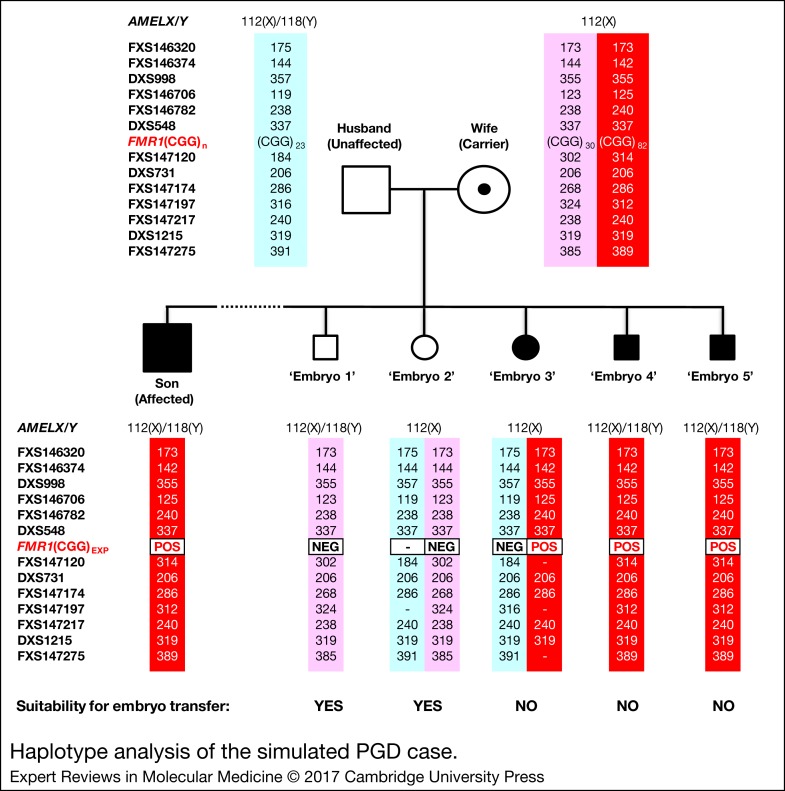
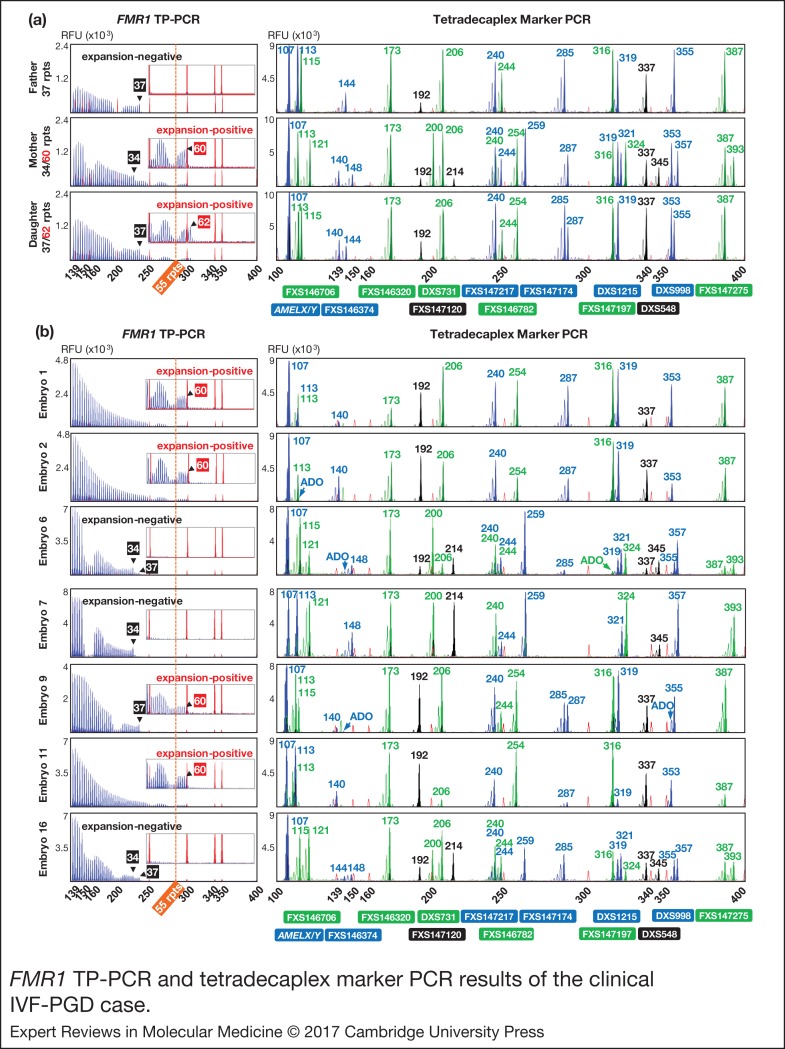
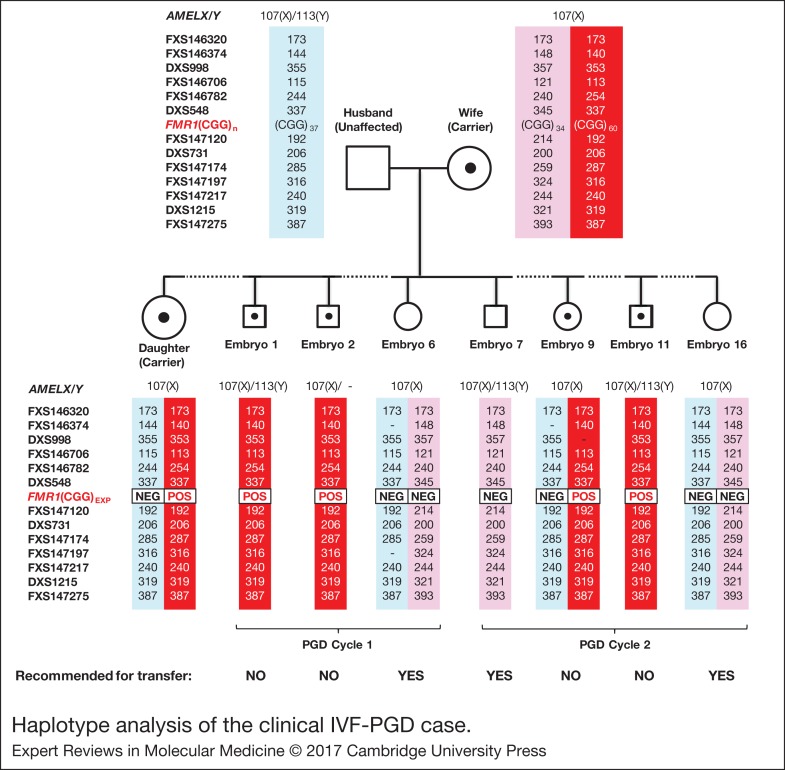
Fragile X mental retardation 1 (FMR1) full-mutation expansion causes fragile X syndrome. Trans-generational fragile X syndrome transmission can be avoided by preimplantation genetic diagnosis (PGD). We describe a robust PGD strategy that can be applied to virtually any couple at risk of transmitting fragile X syndrome. This novel strategy utilises whole-genome amplification, followed by triplet-primed polymerase chain reaction (TP-PCR) for robust detection of expanded FMR1 alleles, in parallel with linked multi-marker haplotype analysis of 13 highly polymorphic microsatellite markers located within 1 Mb of the FMR1 CGG repeat, and the AMELX/Y dimorphism for gender identification. The assay was optimised and validated on single lymphoblasts isolated from fragile X reference cell lines, and applied to a simulated PGD case and a clinical in vitro fertilisation (IVF)-PGD case. In the simulated PGD case, definitive diagnosis of the expected results was achieved for all 'embryos'. In the clinical IVF-PGD case, delivery of a healthy baby girl was achieved after transfer of an expansion-negative blastocyst. FMR1 TP-PCR reliably detects presence of expansion mutations and obviates reliance on informative normal alleles for determining expansion status in female embryos. Together with multi-marker haplotyping and gender determination, misdiagnosis and diagnostic ambiguity due to allele dropout is minimised, and couple-specific assay customisation can be avoided.
Figures
References
-
- Verkerk A.J. et al. (1991) Identification of a gene (FMR-1) containing a CGG repeat coincident with a breakpoint cluster region exhibiting length variation in fragile X syndrome. Cell 65, 905-914 - PubMed
-
- Oberle I. et al. (1991) Instability of a 550-base pair DNA segment and abnormal methylation in fragile X syndrome. Science 252, 1097-1102 - PubMed
-
- Yu S. et al. (1991) Fragile X genotype characterized by an unstable region of DNA. Science 252, 1179-1181 - PubMed
-
- Hill M.K. et al. (2010) A systematic review of population screening for fragile X syndrome. Genetics in Medicine 12, 396-410 - PubMed
-
- Monaghan K.G. et al. (2013) ACMG standards and guidelines for fragile X testing: a revision to the disease-specific supplements to the Standards and Guidelines for Clinical Genetics Laboratories of the American College of Medical Genetics and Genomics. Genetics in Medicine 15, 575-586 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
