

Squamous intraepithelial lesions of the anal squamocolumnar junction: Histopathological classification and HPV genotyping
- PMID: 28720443
- PMCID: PMC5883205
- DOI: 10.1016/j.pvr.2016.12.001
Squamous intraepithelial lesions of the anal squamocolumnar junction: Histopathological classification and HPV genotyping
Abstract
Background: Human papillomavirus (HPV)-related anal cancer lesions are often found adjacent to the squamocolumnar junction (SCJ). We have assessed the histopathology and associated HPV genotypes in anal SCJ lesions in surgically excised anal warts in HIV-negative and -positive patients.
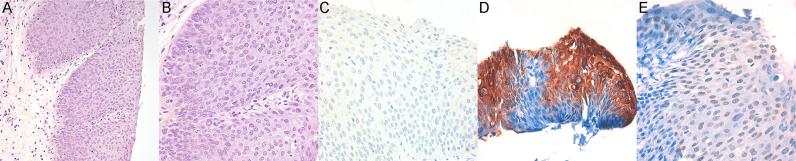
Methods: Histopathology identified 47 squamous intraepithelial lesions (SILs) adjacent to the SCJ amongst a total of 145 cases of clinically diagnosed anal condylomata. The anal SCJ lesions were further analyzed with p16, CK7 and p63 immunohistochemistry and HPV genotyping.
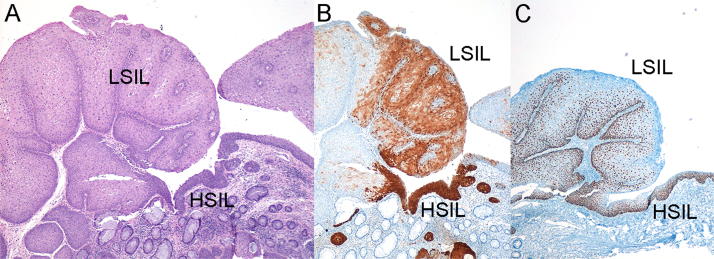
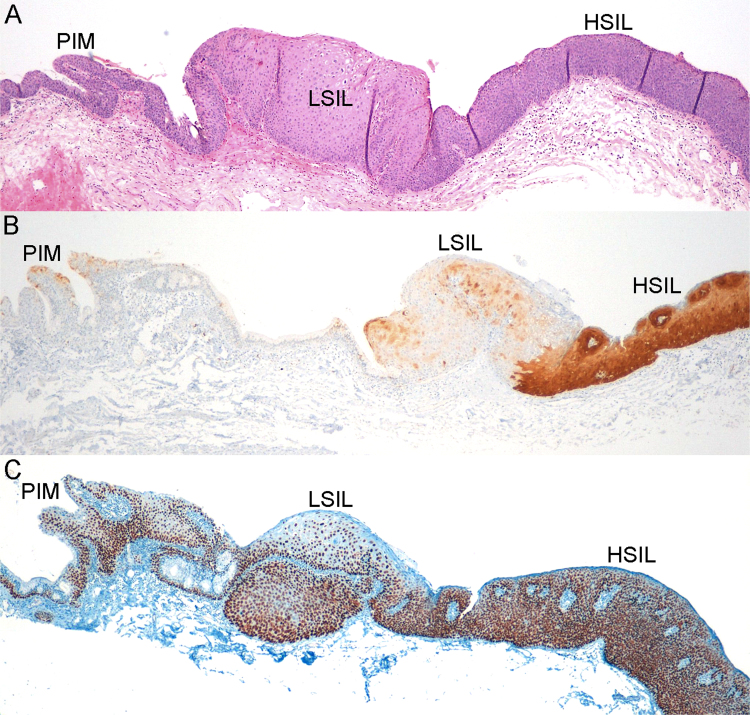
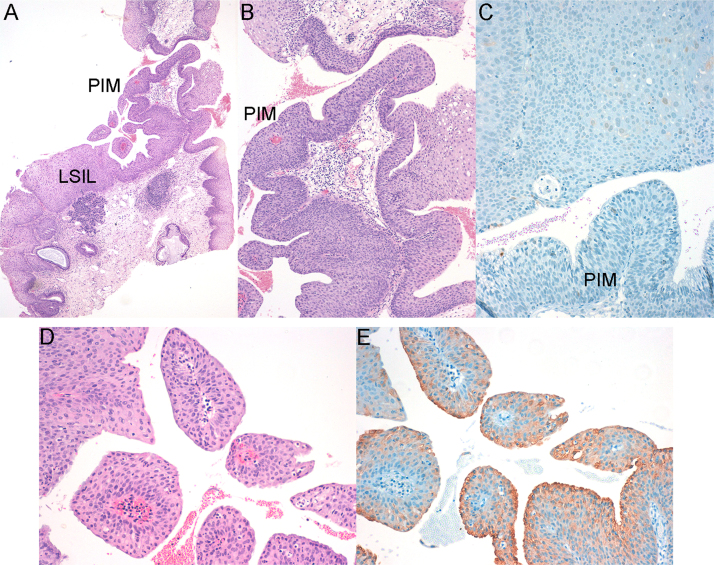
Results: Sixteen (16/47) of the excised anal wart lesions contained HSIL; Three were HSIL and exclusively associated with oncogenic HPVs. A further thirteen (13/47) were mixed lesions. Of these eight were HSILs with LSIL and six were HSILs with papillary immature metaplasia (PIM); Ten of the mixed lesions were associated with one or more oncogenic HPVs, while three cases were exclusively associated with HPV6.
Conclusions: Clinically diagnosed anal warts cannot be assumed to be limited to low-grade lesions as anal warts of the SCJ often show heterogeneous lesions, with coexistence of LSIL, PIM, and HSIL. Lesions showing PIM, however, may mimic HSIL, because they are hypercellular, but lack the nuclear atypia and conspicuous mitotic activity of HSIL; and are p16 negative.
Keywords: Anal squamocolumnar junction; HIV; HPV; High-grade squamous intraepithelial lesion (HSIL); Low-grade squamous intraepithelial lesion (LSIL); Papillary immature metaplasia (PIM).
Copyright © 2016 The Authors. Published by Elsevier B.V. All rights reserved.
Figures

Similar articles
-
A Review and Update on Papillary Immature Metaplasia of the Uterine Cervix: A Distinct Subset of Low-Grade Squamous Intraepithelial Lesion, Proposing a Possible Cell of Origin.Arch Pathol Lab Med. 2018 Aug;142(8):973-981. doi: 10.5858/arpa.2017-0267-OA. Epub 2018 Apr 13. Arch Pathol Lab Med. 2018. PMID: 29652189
-
Predictive Value of Cytokeratin 7 Immunohistochemistry in Cervical Low-grade Squamous Intraepithelial Lesion as a Marker for Risk of Progression to a High-grade Lesion.Am J Surg Pathol. 2016 Feb;40(2):236-43. doi: 10.1097/PAS.0000000000000548. Am J Surg Pathol. 2016. PMID: 26551618
-
Cervical squamocolumnar junction-specific markers define distinct, clinically relevant subsets of low-grade squamous intraepithelial lesions.Am J Surg Pathol. 2013 Sep;37(9):1311-8. doi: 10.1097/PAS.0b013e3182989ee2. Am J Surg Pathol. 2013. PMID: 24076771 Free PMC article.
-
Immunohistochemistry and in situ hybridization for the diagnosis and classification of squamous lesions of the anogenital region.Semin Diagn Pathol. 2015 Sep;32(5):409-18. doi: 10.1053/j.semdp.2015.02.015. Epub 2015 Feb 7. Semin Diagn Pathol. 2015. PMID: 25862555 Review.
-
Anal Cancer in High-Risk Women: The Lost Tribe.Cancers (Basel). 2022 Dec 22;15(1):60. doi: 10.3390/cancers15010060. Cancers (Basel). 2022. PMID: 36612055 Free PMC article. Review.
Cited by
-
Detection of Five Types of HPV Genotypes Causing Anogenital Warts (Condyloma Acuminatum) Using PCR-Tm Analysis Technology.Front Microbiol. 2022 May 17;13:857410. doi: 10.3389/fmicb.2022.857410. eCollection 2022. Front Microbiol. 2022. PMID: 35655998 Free PMC article.
-
Investigation of frequency and typing of human papillomavirus among genital warts using a reverse dot blot hybridization approach.BMC Infect Dis. 2022 Mar 22;22(1):278. doi: 10.1186/s12879-022-07276-8. BMC Infect Dis. 2022. PMID: 35317740 Free PMC article.
-
Prevalence and genotype distribution of HPV6/11/16/18 infections among 180,276 outpatient females from a Women's and Children's Central Hospital, 2015-2021, Chengdu, China.Sci Rep. 2023 Dec 14;13(1):22249. doi: 10.1038/s41598-023-48222-1. Sci Rep. 2023. PMID: 38097632 Free PMC article.
-
Analogies between HPV Behavior in Oral and Vaginal Cavity: Narrative Review on the Current Evidence in the Literature.J Clin Med. 2024 Mar 1;13(5):1429. doi: 10.3390/jcm13051429. J Clin Med. 2024. PMID: 38592283 Free PMC article. Review.
-
A Novel Model for Papillomavirus-Mediated Anal Disease and Cancer Using the Mouse Papillomavirus.mBio. 2021 Aug 31;12(4):e0161121. doi: 10.1128/mBio.01611-21. Epub 2021 Jul 20. mBio. 2021. PMID: 34281391 Free PMC article.
References
-
- J.K. Greenson, ed., Diagnostic Pathology Gastrointestinal, First Ed., Amirsys, Salt Lake City, Utah, 2010.
-
- Johnson L.G., Madeleine M.M., Newcomer L.M., Schwartz S.M., Daling J.R. Anal cancer incidence and survival: the surveillance, epidemiology, and end results experience, 1973–2000. Cancer. 2004;101:281–288. - PubMed
-
- Palefsky J.M., Giuliano A.R., Goldstone S., Moreira E.D., Aranda C., Jessen H., Hillman R., Ferris D., Coutlee F., Stoler M.H., Marshall J.B., Radley D., Vuocolo S., Haupt R.M., Guris D., Garner E.I.O. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N. Engl. J. Med. 2011;365:1576–1585. - PubMed
-
- Fenger C., Bichel P. Flow cytometric DNA analysis of anal canal epithelium and ano-rectal tumours. Acta Microbiol. Scand. A. 1981;89:351–355. 〈http://www.ncbi.nlm.nih.gov/pubmed/7315332〉 (accessed 09.09.14) - PubMed
-
- Abramowitz L., Benabderrahmane D., Ravaud P., Walker F., Rioux C., Jestin C., Bouvet E., Soulé J.-C., Leport C., Duval X. Anal squamous intraepithelial lesions and condyloma in HIV-infected heterosexual men, homosexual men and women: prevalence and associated factors. AIDS. 2007;21:1457–1465. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
