

Effects of Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease: A Systematic Review and Meta-Analysis
- PMID: 28720644
- PMCID: PMC5586302
- DOI: 10.1161/JAHA.117.005835
Effects of Non-Vitamin K Antagonist Oral Anticoagulants Versus Warfarin in Patients With Atrial Fibrillation and Valvular Heart Disease: A Systematic Review and Meta-Analysis
Abstract
Background: The original non-vitamin K antagonist oral anticoagulant (NOAC) trials in nonvalvular atrial fibrillation (AF) enrolled patients with native valve pathologies. The object of this study was to quantify the benefit-risk profiles of NOACs versus warfarin in AF patients with native valvular heart disease (VHD).
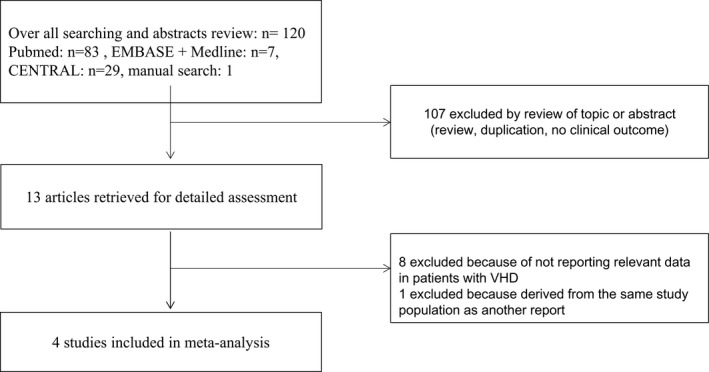
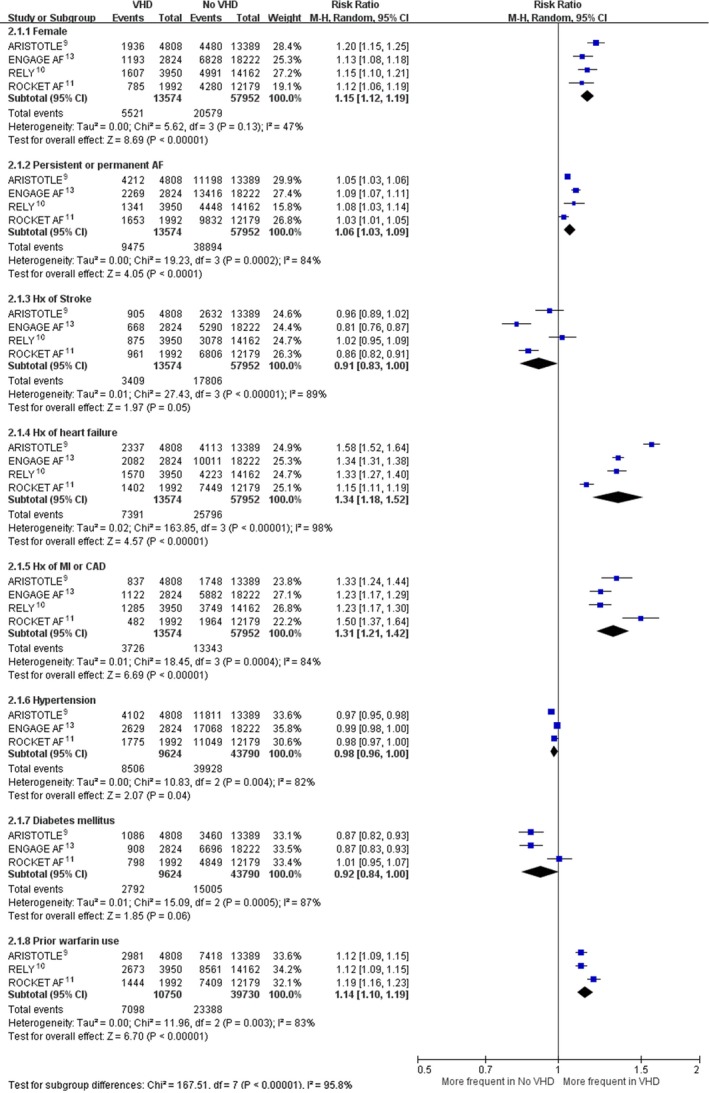
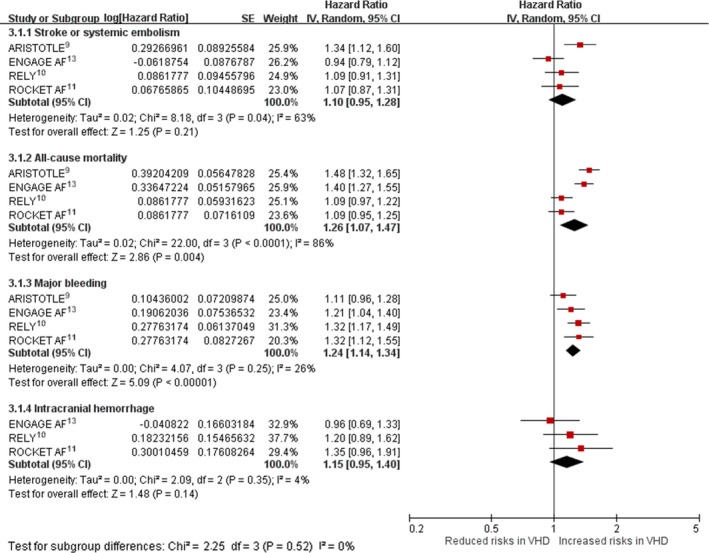
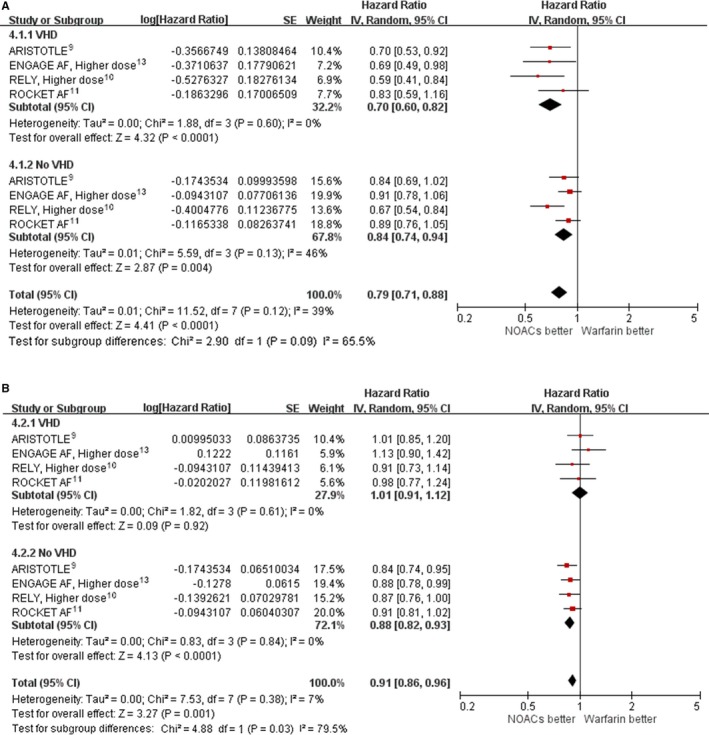
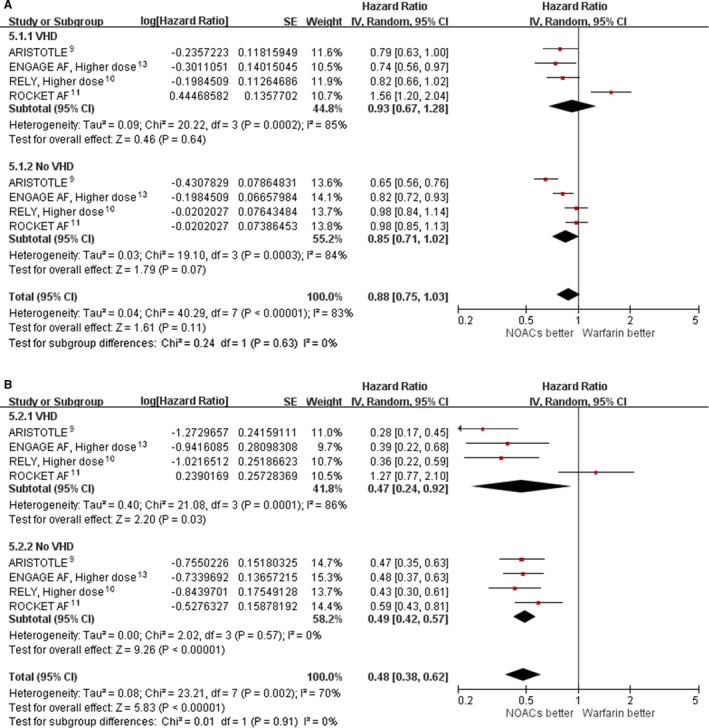
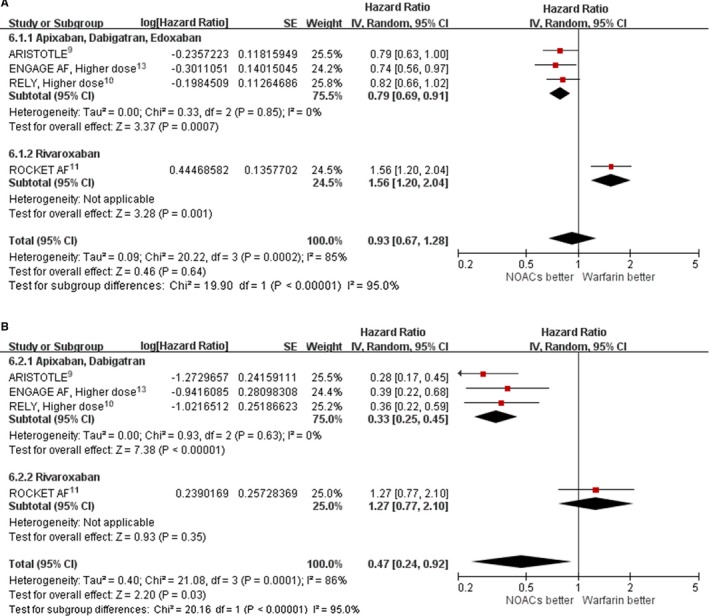
Methods and results: Trials were identified by exhaustive literature search. Trial data were combined using inverse variance weighting to produce a meta-analytic summary hazard ratio (HR) and 95% confidence interval (CI) of efficacy and safety of NOACs versus warfarin. Our final analysis included 4 randomized controlled trials that enrolled 71 526 participants, including 13 574 with VHD. Pooling results from included trials showed that NOACs versus warfarin reduced stroke or systemic embolism (HR: 0.70; 95% CI, 0.60-0.82) and intracranial hemorrhage (HR: 0.47; 95% CI, 0.24-0.92) in AF patients with VHD. However, risk reduction of major bleeding and intracranial hemorrhage was driven by apixaban, edoxaban, and dabigatran (HR for major bleeding: 0.79 [95% CI, 0.69-0.91]; HR for intracranial hemorrhage: 0.33 [95% CI, 0.25-0.45]) but not rivaroxaban (HR for major bleeding: 1.56 [95% CI, 1.20-2.04]; HR for intracranial hemorrhage: 1.27 [95% CI, 0.77-2.10]).
Conclusions: Among patients with AF and native VHD, NOACs reduce stroke and systemic embolism compared with warfarin. Evidence shows that apixaban, dabigatran, and edoxaban also reduce bleeding in this patient subgroup, whereas major bleeding (but not intracranial hemorrhage or mortality rate) is significantly increased in VHD patients treated with rivaroxaban. NOACs are a reasonable alternative to warfarin in AF patients with VHD.
Keywords: anticoagulant; atrial fibrillation; bleeding; stroke; valve.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Wolf PA, Dawber TR, Thomas HE Jr, Kannel WB. Epidemiologic assessment of chronic atrial fibrillation and risk of stroke: the Framingham Study. Neurology. 1978;28:973–977. - PubMed
-
- Brand FN, Abbott RD, Kannel WB, Wolf PA. Characteristics and prognosis of lone atrial fibrillation. 30‐year follow‐up in the Framingham Study. JAMA. 1985;254:3449–3453. - PubMed
-
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983–988. - PubMed
-
- European Heart Rhythm A, European Association for Cardio‐Thoracic S , Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al‐Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369–2429. - PubMed
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, Pogue J, Reilly PA, Themeles E, Varrone J, Wang S, Alings M, Xavier D, Zhu J, Diaz R, Lewis BS, Darius H, Diener HC, Joyner CD, Wallentin L; Committee R‐LS and Investigators . Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139–1151. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
