

Review
doi: 10.1016/j.jcot.2017.06.012.
Epub 2017 Jun 13.
Imaging investigations in Spine Trauma: The value of commonly used imaging modalities and emerging imaging modalities
Affiliations
- PMID: 28720986
- PMCID: PMC5498756
- DOI: 10.1016/j.jcot.2017.06.012
Item in Clipboard
Review
Imaging investigations in Spine Trauma: The value of commonly used imaging modalities and emerging imaging modalities
J Clin Orthop Trauma.
2017 Apr-Jun.
Abstract
Traumatic spine injuries can be devastating for patients affected and for health care professionals if preventable neurological deterioration occurs. This review discusses the imaging options for the diagnosis of spinal trauma. It lays out when imaging is appropriate and when it is not. It discusses strength and weakness of available imaging modalities. Advanced techniques for spinal injury imaging will be explored. The review concludes with a review of imaging protocols adjusted to clinical circumstances.
Keywords: CT; Guideline; Imaging; MRI; Protocol; Radiography; Spine imaging; Spine injury; Spine stability; Spine trauma.
Figures
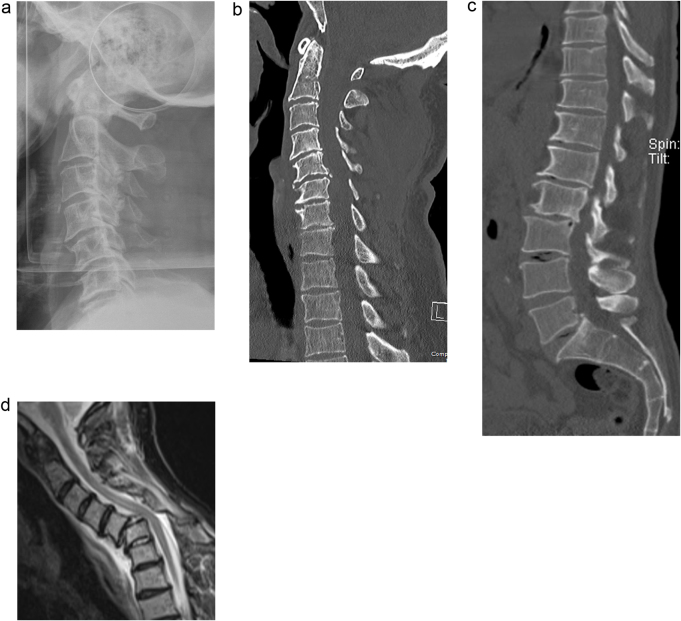
79 year old male, fall. Cervical spine radiographs (shown lateral cervical spine, figure a), CT cervical spine (shown sagittal reformat, figure b) and CT of the abdomen and pelvis (shown sagittal reformat, figure c), have not demonstrated a bone injury. Malalignment and subluxation at the C5/6 level was not appreciated as relevant. Cervical instability and neurological symptoms instigated repeat radiographs demonstrating instability and triggering MRI referral. MRI (figure d, sagittal STIR image) confirms marked subluxation at the C5/6 level and cord signal change indicating oedema. CT can not diagnose neural injury and may not exclude instability.
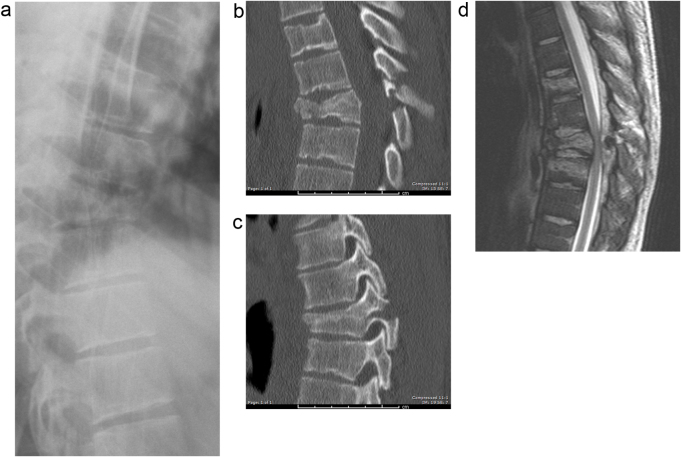
24 year old male, mountain bike accident. Lumbar and thoracic spine radiographs were obtained and show a T8 fracture with anterior wedging (figure a, lateral radiograph T-spine). CT was performed for further characterisation, a crush fracture of the vertebral body and disruption of the posterior elements was seen (figure b, midsagittal reformat; figure c parasagittal). This is clearly an unstable injury. CT is excellent for depicting extent and nature of bone injury and here determines an unstable injury. MR imaging (figure d, sagittal T2w) shows epidural haematoma with cord compromise, this can not be appreciated on CT. Bicycle injuries carry a high risk for spinal injury.
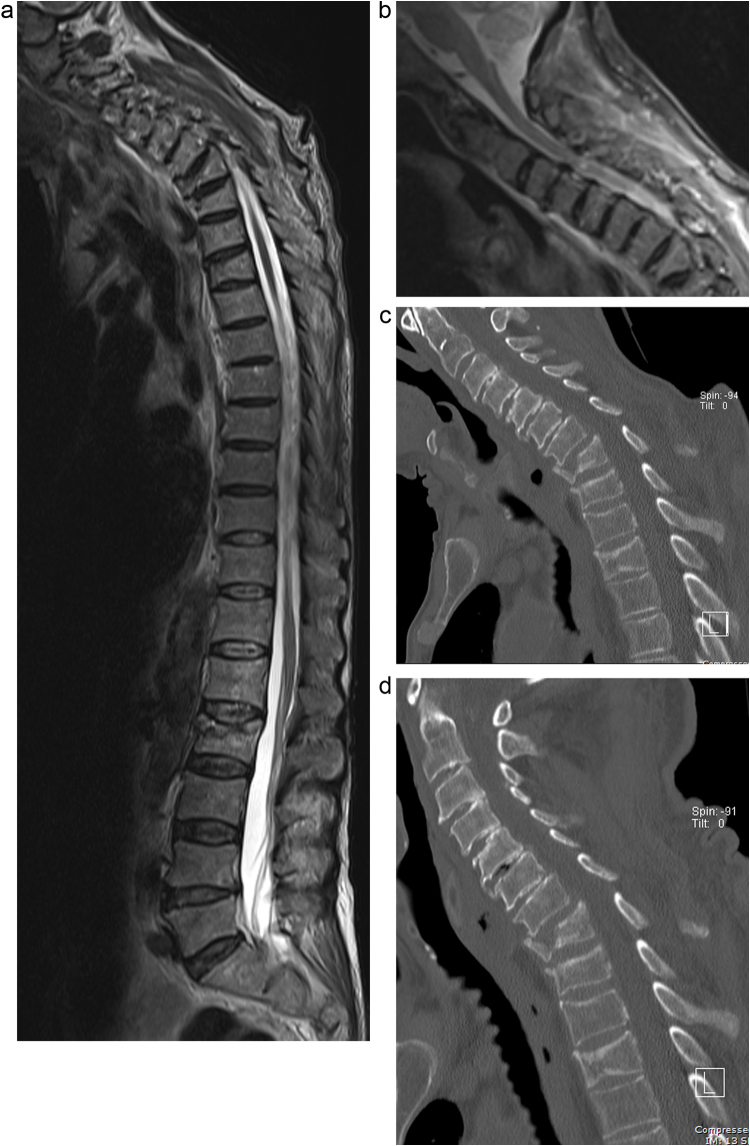
87 year old male, fall. T2weighted MRI of the whole spine demonstrates multilevel fractures, in the upper and mid thoracic spine and in the upper lumbar spine (figure a). Sagittal STIR images of the cervical spine show focal cord signal change at the C4 level, pre-existing OA, typical central cord injury in an elderly patient with pre-existing OA and no evidence of instability (image b). Flexion (image c) and extension (image d) CT images show no evidence of instability. CT can not directly visualise neural injury. Multilevel injuries of the spine are common.
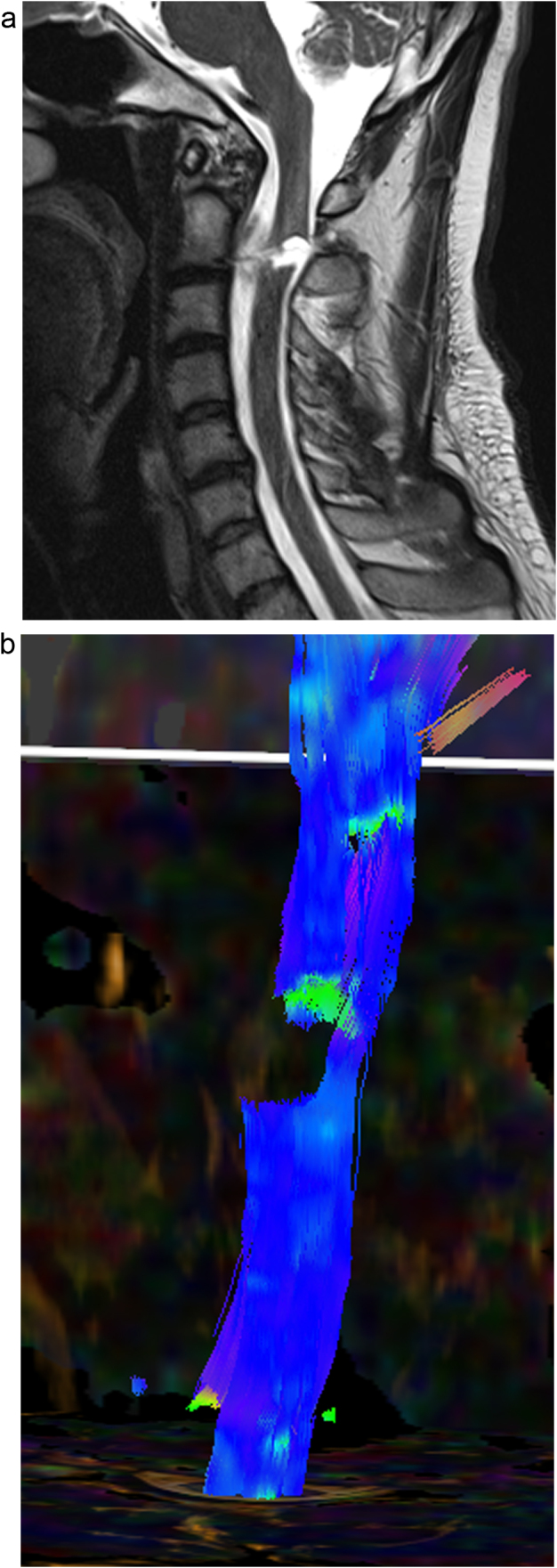
26 year old male, knife injury to the C2/3 level. Sagittal T2 w MRI images (figure a) show partial transection of the cervical spinal cord. Tractography (image b, posterior projection) confirms the injury. However diffusion weighted imaging does not add any significant new information.
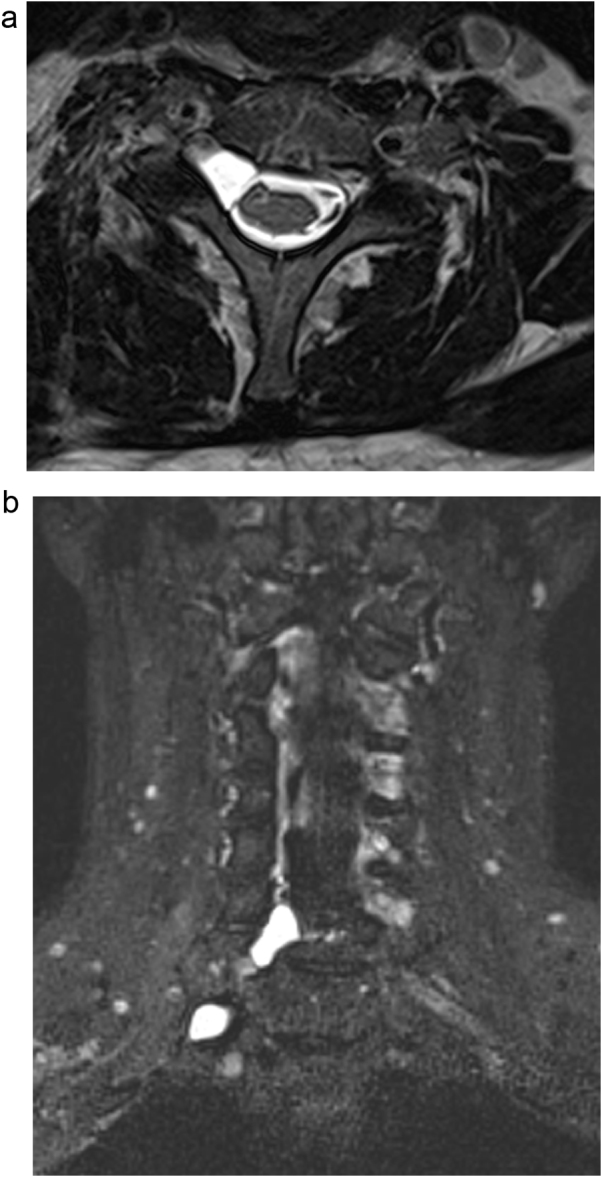
41 year old man with brachial plexus injury. Axial T2 space and coronal space STIR images show absent right sided rootlets (figure a) and menigocele formation (figure b). MRI is able to directly visualise rootlet injuries of the spine.
References
-
- Gerrelts B.D., Petersen E.U., Mabry J., Petersen S.R. Delayed diagnosis of cervical spine injuries. J Trauma. 1991;31:1622–1626. - PubMed
-
- Davis J.W., Phreaner D.L., Hoyt D.B., Mackersie R.C. The etiology of missed cervical spine injuries. J Trauma. 1993;34:342–346. - PubMed
-
- Poonnoose P.M., Ravichandran G., McClelland M.R. Missed and mismanaged injuries of the spinal cord. J Trauma. 2002;53:314–320. - PubMed
-
- Reid D.C., Henderson R., Saboe L., Miller J.D. Etiology and clinical course of missed spine fractures. J Trauma. 1987;27:980–986. - PubMed
-
- El Fegoun A.B., Staccini P., Gille O., de Peretti F. Delayed diagnosis of inferior cervical spine injury. Rev Chir Orthop Reparatrice Appar Mot. 2004;90:517–524. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
