

Final Report of a Prospective Randomized Trial to Evaluate the Dose-Response Relationship for Postoperative Radiation Therapy and Pathologic Risk Groups in Patients With Head and Neck Cancer
- PMID: 28721881
- PMCID: PMC5518636
- DOI: 10.1016/j.ijrobp.2017.02.218
Final Report of a Prospective Randomized Trial to Evaluate the Dose-Response Relationship for Postoperative Radiation Therapy and Pathologic Risk Groups in Patients With Head and Neck Cancer
Abstract
Purpose: To present the long-term and final report of a phase 3 trial designed to assess dose-response relationship for postoperative radiation therapy (PORT) and pathologic risk groups in head and neck cancer.
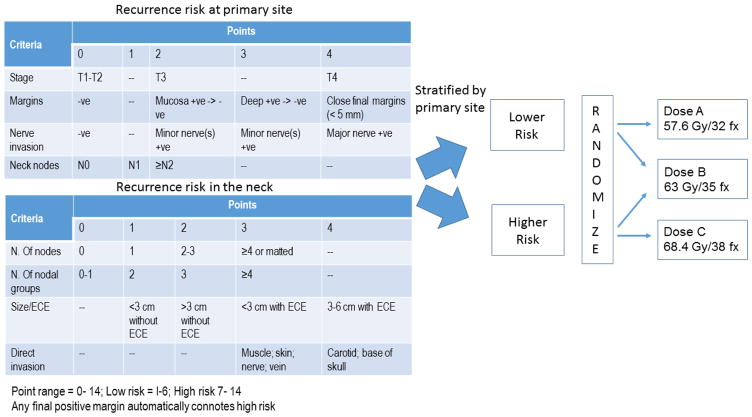
Methods and materials: Patients who underwent primary surgery for American Joint Committee on Cancer stage III or IV squamous cell carcinoma of the oral cavity, oropharynx, hypopharynx, or larynx and who required PORT were eligible. Patients' primary sites and involved necks were independently assigned to higher- or lower-risk categories based on a cumulative point score representing increasing risk of recurrence. The sites in the lower-risk group were randomized to receive 57.6 or 63 Gy and those in the higher-risk group were randomized to receive 63 or 68.4 Gy, all at 1.8 Gy per fraction.
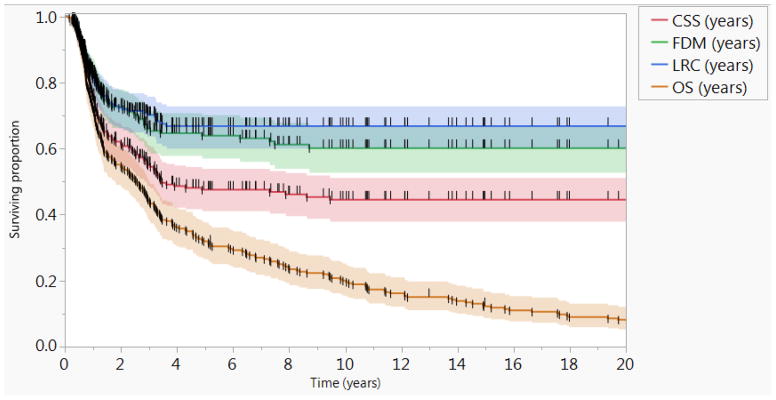
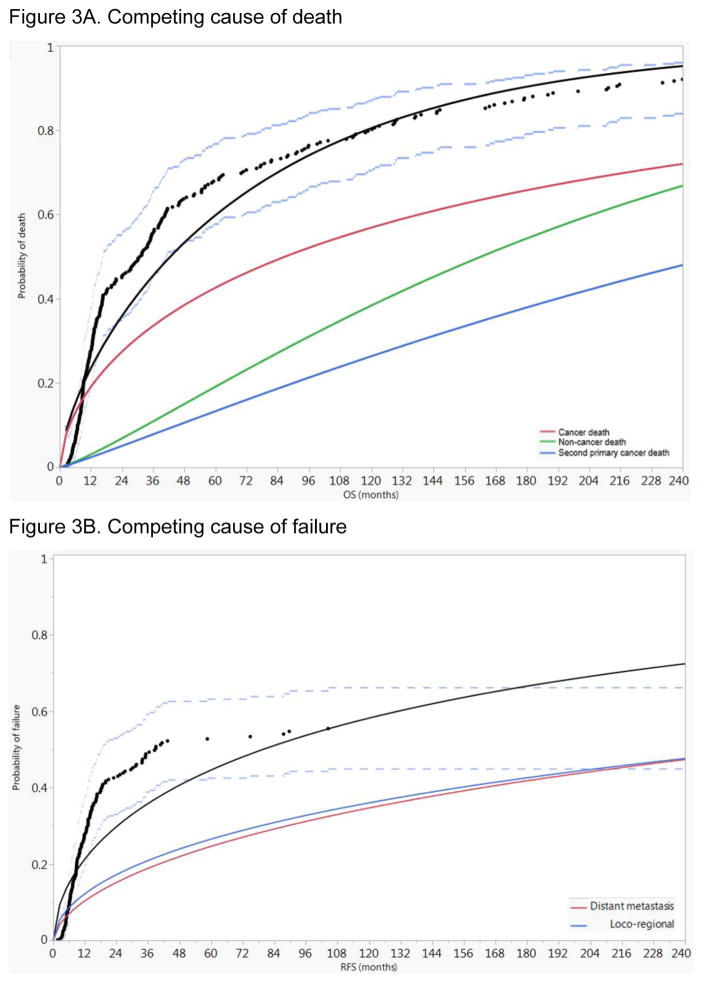
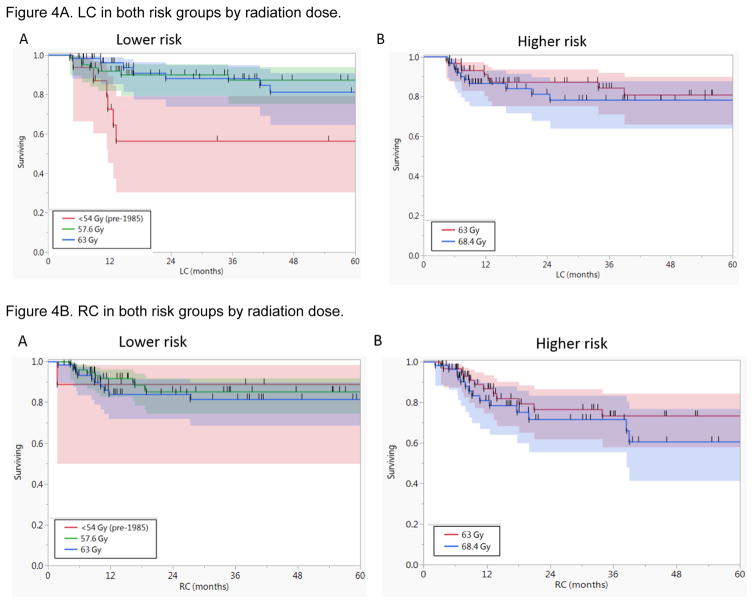
Results: A total of 264 patients were included. The actuarial 5-year locoregional control rate was 67%. A second primary cancer was documented in 27% of patients. The 5- and 10-year freedom-from-distant metastasis rates were 64% and 60%, respectively, whereas the 5- and 10-year overall survival rates were 32% and 20%, respectively. There was no statistically significant difference in tumor control between different dose levels in both the lower- and higher-risk groups. On multivariate analysis, nonwhite race (P=.0003), positive surgical margins (P=.009), extracapsular extension (ECE, P=.01), and treatment package time (TPT) ≥85 days (P=.002) were independent correlates of worse locoregional control, whereas age ≥57 years (P<.0001), positive surgical margins (P=.01), ECE (P=.026), and TPT ≥85 days (P=.003) were independently associated with worse overall survival.
Conclusions: This long-term report of PORT delivered at 1.8 Gy/d to total doses of 57.6 to 68.4 Gy without chemotherapy for head and neck squamous cell carcinoma demonstrated that increasing dose did not significantly improve tumor control. On multivariate analysis, the only significant treatment variable was TPT. The results confirm that positive surgical margins and/or nodal ECE remains the most significant predictive pathologic factors.
Copyright © 2017 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Why So Challenging to Personalize Radiation Dose?Int J Radiat Oncol Biol Phys. 2017 Aug 1;98(5):1012-1013. doi: 10.1016/j.ijrobp.2017.03.021. Epub 2017 Jul 10. Int J Radiat Oncol Biol Phys. 2017. PMID: 28721882 No abstract available.
References
-
- Maccomb WS, Fletcher GH. Planned combination of surgery and radiation in treatment of advanced primary head and neck cancers. The American journal of roentgenology, radium therapy, and nuclear medicine. 1957;77:397–414. - PubMed
-
- Feldman M, Fletcher GH. Analysis of the parameters relating to failures above the clavicles in patients treated by postoperative irradiation for squamous cell carcinomas of the oral cavity or oropharynx. International journal of radiation oncology, biology, physics. 1982;8:27–30. - PubMed
-
- Barkley HT, Fletcher GH, Jesse RH, Lindberg RD. Papers of the First Joint Meeting of the American Radium Society, James Ewing Society, and the Society of Head and Neck Surgeons Management of cervical lymph node metastases in squamous cell carcinoma of the tonsillar fossa, base of tongue, supraglottic larynx, and hypopharynx. The American Journal of Surgery. 1972;124:462–7. - PubMed
-
- Vikram B, Strong EW, Shah JP, Spiro R. Failure at the primary site following multimodality treatment in advanced head and neck cancer. Head & neck surgery. 1984;6:720–3. - PubMed
-
- Bartelink H, Breur K, Hart G, Annyas B, van Slooten E, Snow G. The value of postoperative radiotherapy as an adjuvant to radical neck dissection. Cancer. 1983;52:1008–13. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
