

Assessing the Generalizability of the National Lung Screening Trial: Comparison of Patients with Stage 1 Disease
- PMID: 28722466
- PMCID: PMC5803664
- DOI: 10.1164/rccm.201705-0914OC
Assessing the Generalizability of the National Lung Screening Trial: Comparison of Patients with Stage 1 Disease
Abstract
Rationale: The findings of the NLST (National Lung Screening Trial) are the basis for screening high-risk individuals according to age and smoking history. Although screening is covered for eligible Medicare beneficiaries, the generalizability of the NLST in the elderly population has been questioned.
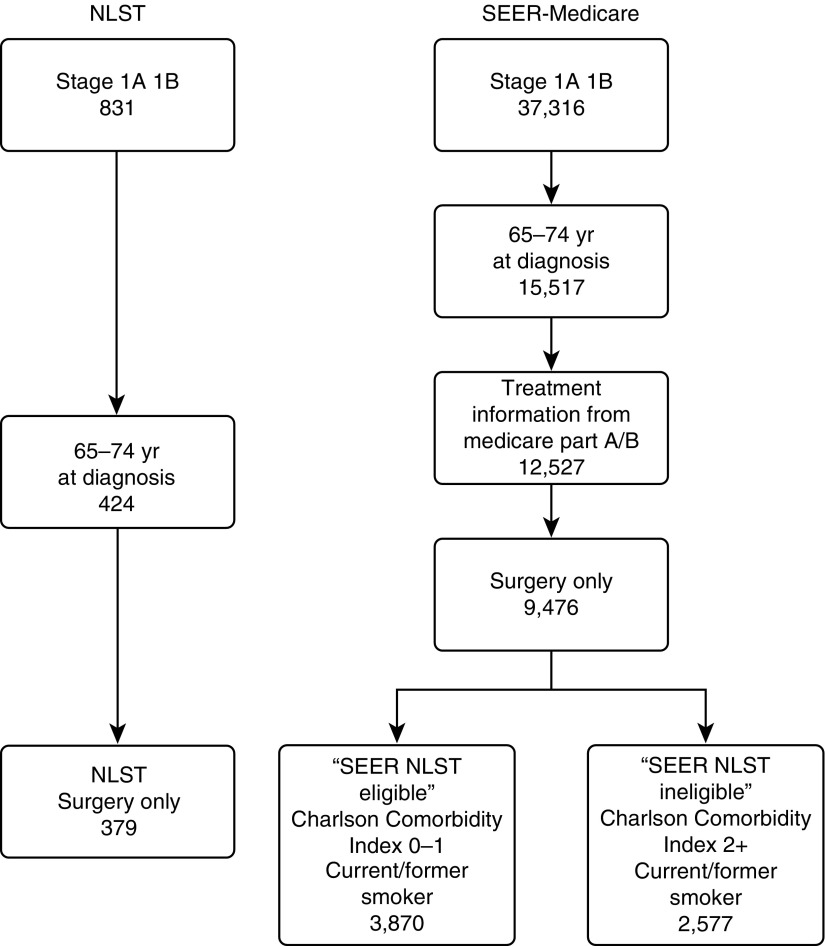
Objectives: Compare outcomes of patients diagnosed with stage 1 non-small cell lung cancer in the NLST to a nationally representative cohort of elderly patients Methods: Analysis of Surveillance, Epidemiology, and End Results (SEER)-Medicare and NLST datasets for patients with stage 1 disease aged 65 to 74 years.
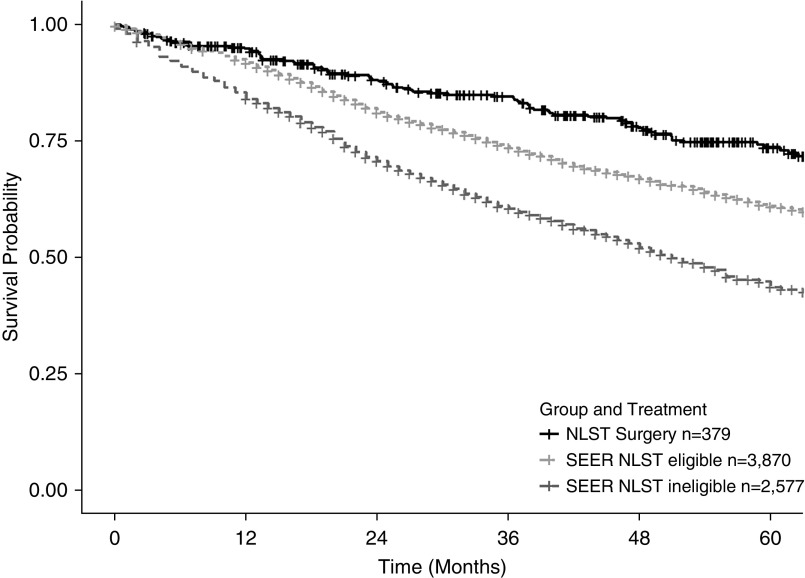
Measurements and main results: Lung cancer-specific mortality, all-cause mortality, and 30-, 60-, and 90-day treatment mortality were measured. When compared with the NLST group undergoing surgery for stage 1 non-small cell lung cancer, those in the SEER-Medicare NLST eligible cohort had no difference in adjusted odds ratios for 30-, 60-, and 90-day surgical mortality (P values = 0.97, 0.65, and 0.46, respectively). Although the 5-year cancer-specific survival did not differ between cohorts (hazard ratio [HR], 0.84 NLST vs. SEER-Medicare NLST eligible; P = 0.21), the adjusted HR estimate for all-cause mortality was better in the NLST cohort (HR, 0.71; P < 0.01). For patients who did not receive surgery for early-stage disease (presumably for curative intent), the outcomes were far worse (13.1, 18.9, 23.9%, for 30-, 60-, and 90-day treatment mortality, respectively).
Conclusions: Elderly patients with minimal comorbid conditions meeting the inclusion criteria of the NLST who underwent surgery had excellent postoperative outcomes and similar lung cancer-specific 5-year survivorship. In those with significant comorbidities or those not undergoing surgery, competing causes of death may diminish the benefit, and there is no evidence to recommend screening in this group.
Keywords: comorbidities; lung cancer screening; stage 1 lung cancer outcomes.
Figures
Comment in
-
Young at Heart: Is That Good Enough for Computed Tomography Screening?Am J Respir Crit Care Med. 2017 Sep 1;196(5):539-541. doi: 10.1164/rccm.201707-1504ED. Am J Respir Crit Care Med. 2017. PMID: 28806529 No abstract available.
References
-
- Hendrick RE, Helvie MA. Mammography screening: a new estimate of number needed to screen to prevent one breast cancer death. AJR Am J Roentgenol. 2012;198:723–728. - PubMed
-
- Goldstraw P, Crowley J, Chansky K, Giroux DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V, Sobin L International Association for the Study of Lung Cancer International Staging Committee; Participating Institutions. The IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumours. J Thorac Oncol. 2007;2:706–714. - PubMed
-
- Boffa DJ, Allen MS, Grab JD, Gaissert HA, Harpole DH, Wright CD. Data from The Society of Thoracic Surgeons General Thoracic Surgery database: the surgical management of primary lung tumors. J Thorac Cardiovasc Surg. 2008;135:247–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
