

Evolution of anti-Trypanosoma cruzi antibody production in patients with chronic Chagas disease: Correlation between antibody titers and development of cardiac disease severity
- PMID: 28723905
- PMCID: PMC5536389
- DOI: 10.1371/journal.pntd.0005796
Evolution of anti-Trypanosoma cruzi antibody production in patients with chronic Chagas disease: Correlation between antibody titers and development of cardiac disease severity
Abstract
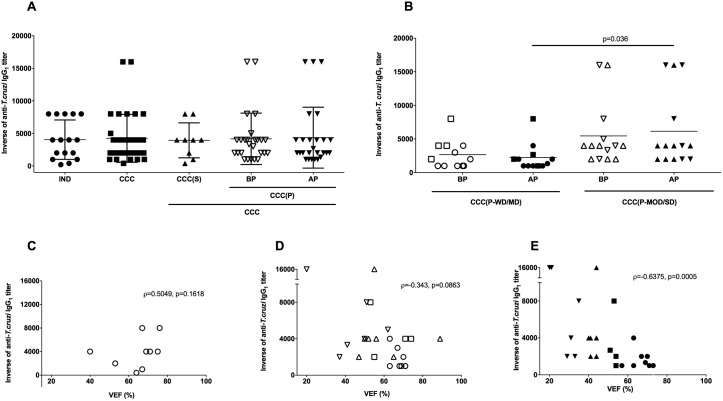
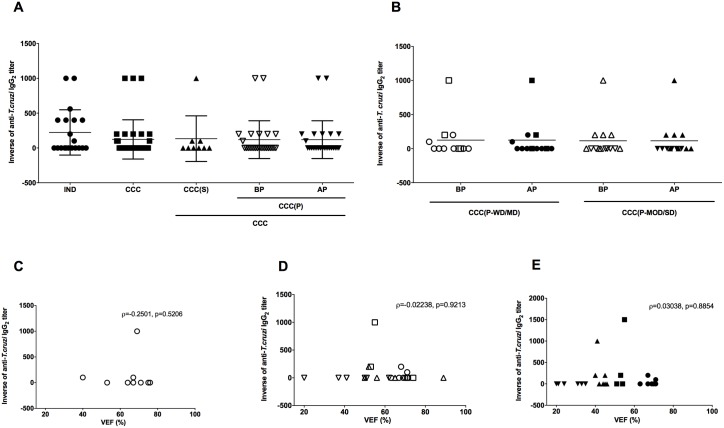
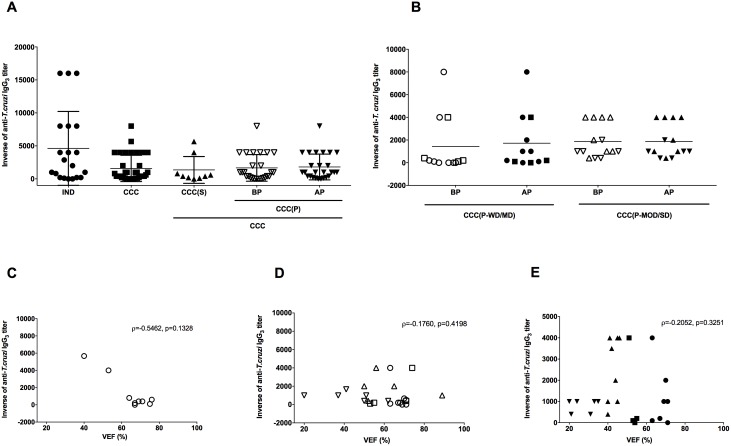
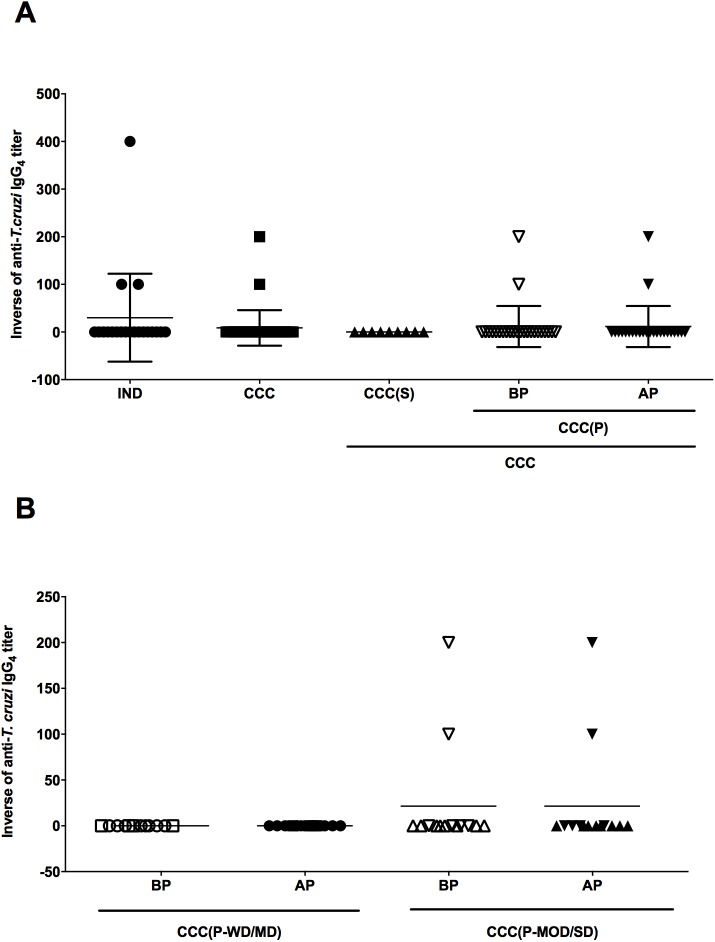
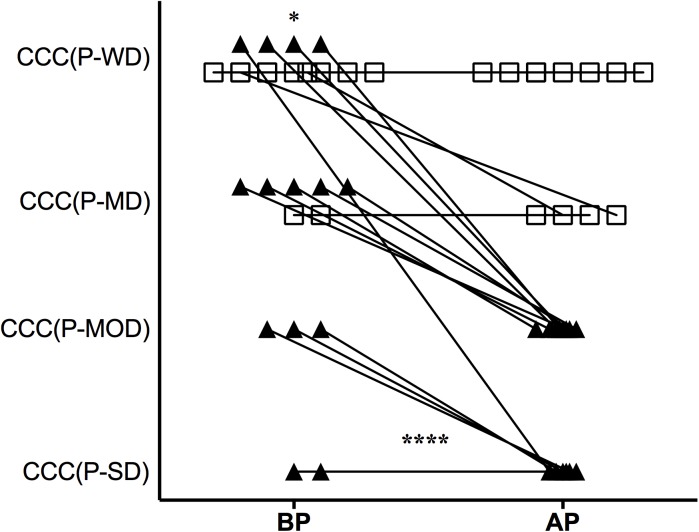
Chagas disease is one of the most important endemic infections in Latin America affecting around 6-7 million people. About 30-50% of patients develop the cardiac form of the disease, which can lead to severe cardiac dysfunction and death. In this scenario, the identification of immunological markers of disease progression would be a valuable tool for early treatment and reduction of death rates. In this observational study, the production of anti-Trypanosoma cruzi antibodies through a retrospective longitudinal follow-up in chronic Chagas disease patients´ cohort and its correlation with disease progression and heart commitment was evaluated. Strong inverse correlation (ρ = -0.6375, p = 0.0005) between anti-T. cruzi IgG1 titers and left ventricular ejection fraction (LVEF) in chronic Chagas cardiomyopathy (CCC) patients were observed after disease progression. Elevated levels of anti-T. cruzi IgG3 titers were detected in all T. cruzi-infected patients, indicating a lack of correlation of this IgG isotype with disease progression. Furthermore, low levels of anti-T. cruzi IgG2, IgG4, and IgA were detected in all patients through the follow-up. Although without statistical significance anti-T. cruzi IgE tends to be more reactive in patients with the indeterminate form (IND) of the disease (p = 0.0637). As this study was conducted in patients with many years of chronic disease no anti-T. cruzi IgM was detected. Taken together, these results indicate that the levels of anti-T. cruzi IgG1 could be considered to seek for promising biomarkers to predict the severity of chronic Chagas disease cardiomyopathy.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- WHO. Chagas disease (American trypanosomiasis) Internet: World Health Organization; 2015 [cited 2016 Nov 19]. Available from: http://www.who.int/mediacentre/factsheets/fs340/en/.
-
- SVSMS. Chagas Disease Technical Information Internet: Brazilian Ministry of Health; 2015 [cited 2016 Nov 19]. Available from: http://portalsaude.saude.gov.br/index.php/o-ministerio/principal/leia-ma....
-
- Shikanai-Yasuda MA, Lopes MH, Tolezano JE, Umezawa E, Amato Neto V, Barreto AC, et al. [Acute Chagas' disease: transmission routes, clinical aspects and response to specific therapy in diagnosed cases in an urban center]. Rev Inst Med Trop Sao Paulo. 1990;32(1):16–27. . - PubMed
-
- Nunes MC, Dones W, Morillo CA, Encina JJ, Ribeiro AL, Council on Chagas Disease of the Interamerican Society of C. Chagas disease: an overview of clinical and epidemiological aspects. J Am Coll Cardiol. 2013;62(9):767–76. doi: 10.1016/j.jacc.2013.05.046 . - DOI - PubMed
-
- Andrade JP, Marin Neto JA, Paola AA, Vilas-Boas F, Oliveira GM, Bacal F, et al. I Latin American Guidelines for the diagnosis and treatment of Chagas' heart disease: executive summary. Arq Bras Cardiol. 2011;96(6):434–42. . - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
