

Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial fibrillation
- PMID: 28724590
- PMCID: PMC5562962
- DOI: 10.1212/WNL.0000000000004235
Long-term antithrombotic treatment in intracranial hemorrhage survivors with atrial fibrillation
Abstract
Objective: To perform a systematic review and meta-analysis of studies reporting recurrent intracranial hemorrhage (ICH) and ischemic stroke (IS) in ICH survivors with atrial fibrillation (AF) during long-term follow-up.
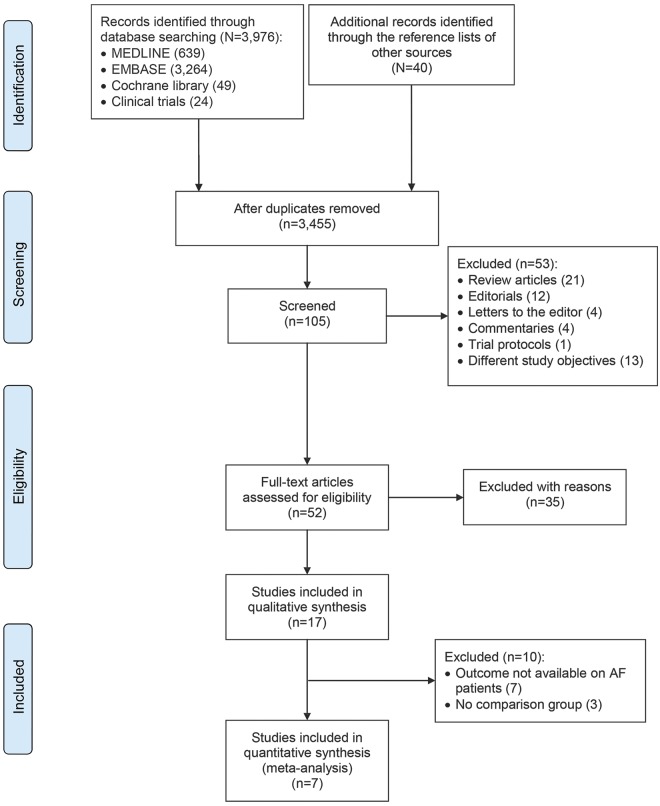
Methods: A comprehensive literature search including MEDLINE, EMBASE, Cochrane library, clinical trials registry was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. We considered studies capturing outcome events (ICH recurrence and IS) for ≥3 months and treatment exposure to vitamin K antagonists (VKAs), antiplatelet agents (APAs), or no antithrombotic medication (no-ATM). Corresponding authors provided aggregate data for IS and ICH recurrence rate between 6 weeks after the event and 1 year of follow-up for each treatment exposure. Meta-analyses of pooled rate ratios (RRs) were conducted with the inverse variance method.
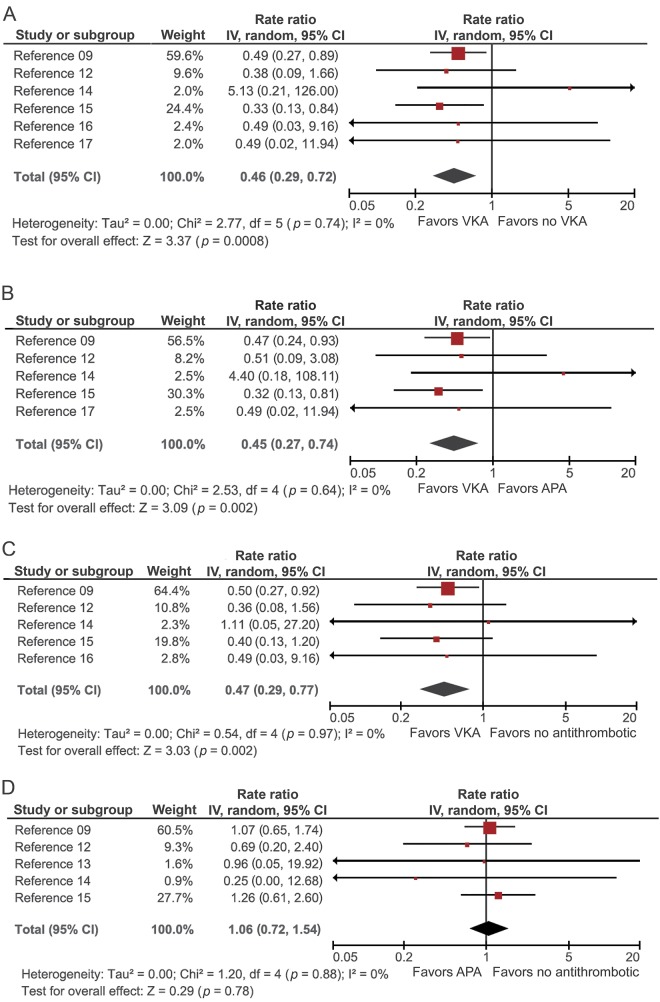
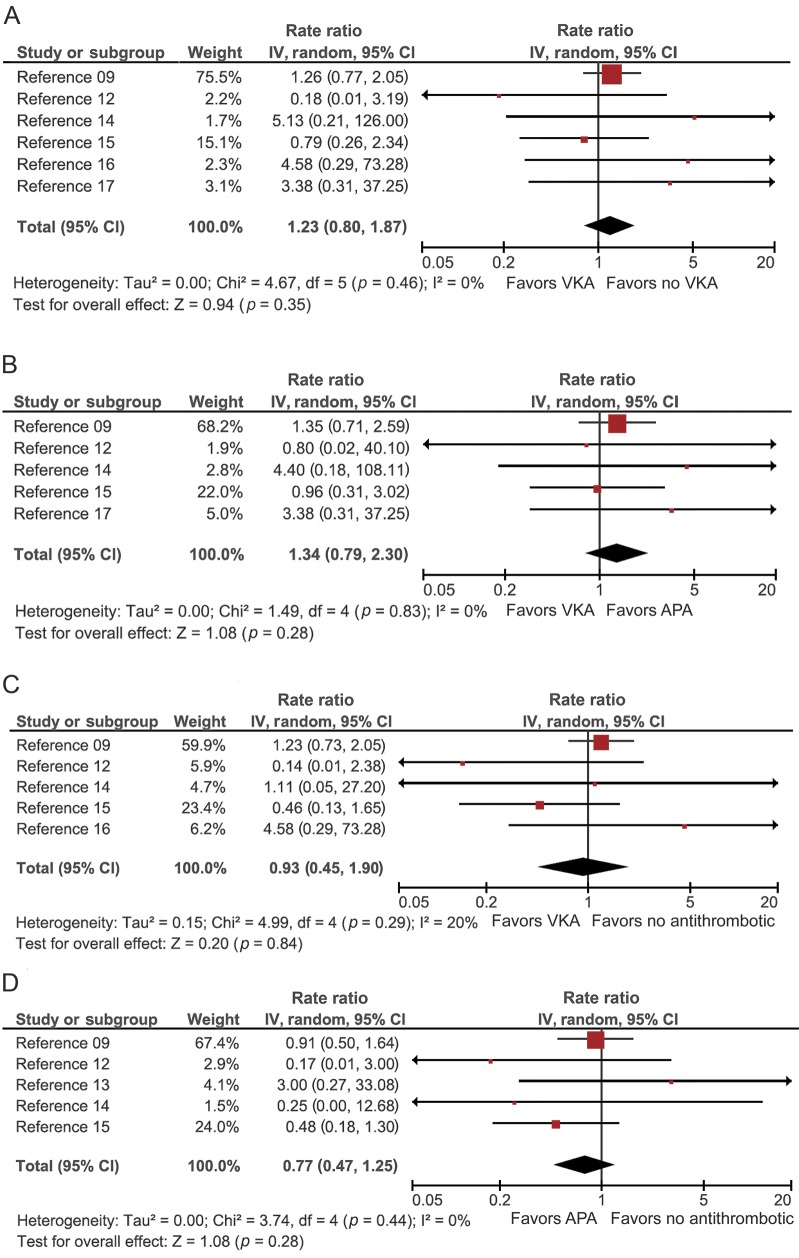
Results: Seventeen articles met inclusion criteria. Seven observational studies enrolling 2,452 patients were included in the meta-analysis. Pooled RR estimates for IS were lower for VKAs compared to APAs (RR = 0.45, 95% confidence interval [CI] 0.27-0.74, p = 0.002) and no-ATM (RR = 0.47, 95% CI 0.29-0.77, p = 0.002). Pooled RR estimates for ICH recurrence were not significantly increased across treatment groups (VKA vs APA: RR = 1.34, 95% CI 0.79-2.30, p = 0.28; VKA vs no-ATM: RR = 0.93, 95% CI 0.45-1.90, p = 0.84).
Conclusions: In observational studies, anticoagulation with VKA is associated with a lower rate of IS than APA or no-ATM without increasing ICH recurrence significantly. A randomized controlled trial is needed to determine the net clinical benefit of anticoagulation in ICH survivors with AF.
© 2017 American Academy of Neurology.
Figures
References
-
- Camm AJ, Lip GY, De Caterina R, et al. 2012 Focused update of the ESC guidelines for the management of atrial fibrillation: an update of the 2010 ESC guidelines for the management of atrial fibrillation: developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012;33:2719–2747. - PubMed
-
- Flynn RW, MacDonald TM, Murray GD, Doney AS. Systematic review of observational research studying the long-term use of antithrombotic medicines following intracerebral hemorrhage. Cardiovasc Ther 2010;28:177–184. - PubMed
-
- Poon MT, Fonville AF, Al-Shahi Salman R. Long-term prognosis after intracerebral haemorrhage: systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2014;85:660–667. - PubMed
-
- Pisters R, Lane DA, Nieuwlaat R, de Vos CB, Crijns HJ, Lip GY. A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey. Chest 2010;138:1093–1100. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous