

Diabetic retinopathy: current understanding, mechanisms, and treatment strategies
- PMID: 28724805
- PMCID: PMC5518557
- DOI: 10.1172/jci.insight.93751
Diabetic retinopathy: current understanding, mechanisms, and treatment strategies
Abstract
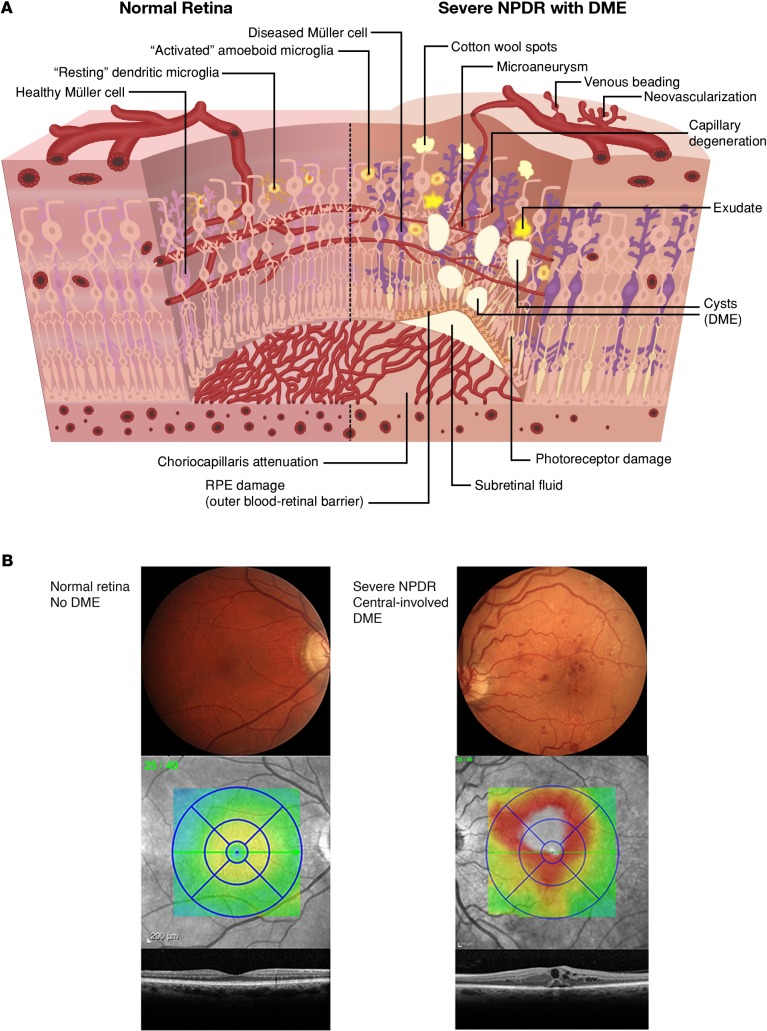
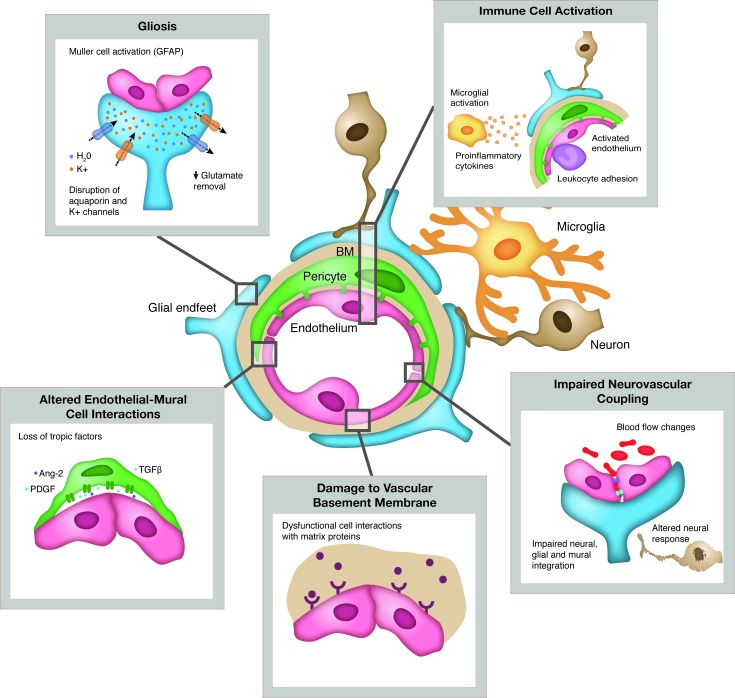
Diabetic retinopathy (DR) causes significant visual loss on a global scale. Treatments for the vision-threatening complications of diabetic macular edema (DME) and proliferative diabetic retinopathy (PDR) have greatly improved over the past decade. However, additional therapeutic options are needed that take into account pathology associated with vascular, glial, and neuronal components of the diabetic retina. Recent work indicates that diabetes markedly impacts the retinal neurovascular unit and its interdependent vascular, neuronal, glial, and immune cells. This knowledge is leading to identification of new targets and therapeutic strategies for preventing or reversing retinal neuronal dysfunction, vascular leakage, ischemia, and pathologic angiogenesis. These advances, together with approaches embracing the potential of preventative or regenerative medicine, could provide the means to better manage DR, including treatment at earlier stages and more precise tailoring of treatments based on individual patient variations.
Conflict of interest statement
Figures
References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
