

Intracranial Hemangiopericytomas: Recurrence, Metastasis, and Radiotherapy
- PMID: 28725519
- PMCID: PMC5515655
- DOI: 10.1055/s-0037-1599073
Intracranial Hemangiopericytomas: Recurrence, Metastasis, and Radiotherapy
Abstract
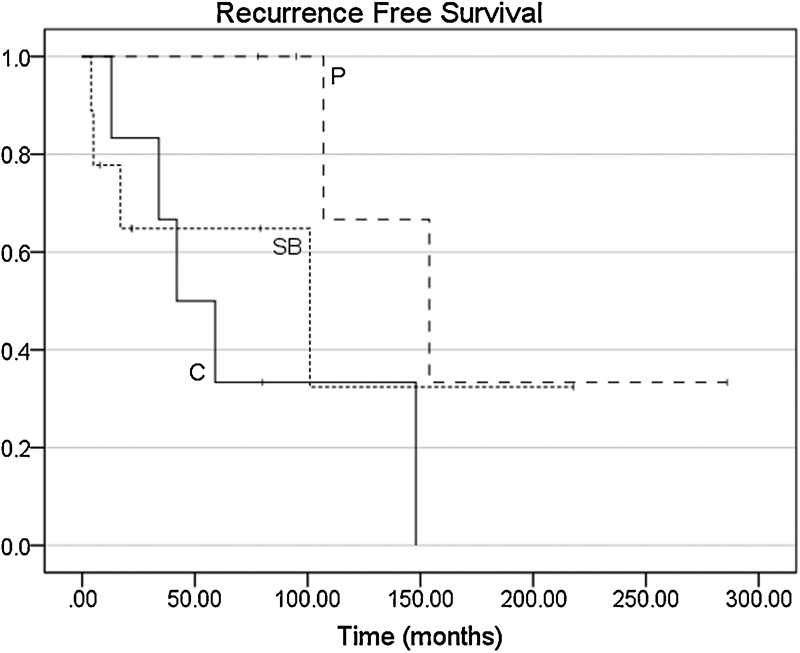
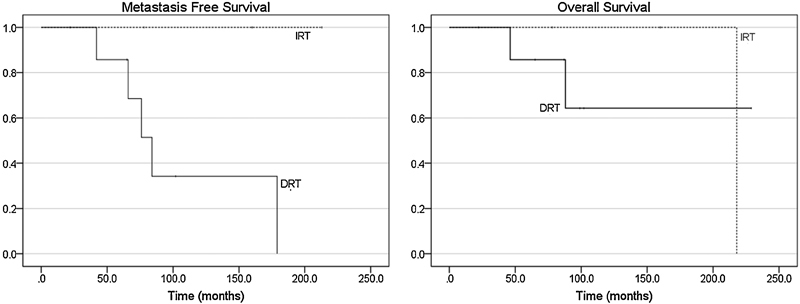
Background Intracranial hemangiopericytomas (HPCs) are characterized by high recurrence rates and extracranial metastases. Radiotherapy provides an adjunct to surgery, but the timing of therapy and the patients most likely to benefit remain unclear. Methods A retrospective review of 20 patients with HPC treated at the University of Texas Southwestern Medical Center between 1985 and 2014 was conducted. Recurrence and metastasis rates along with overall survival (OS) were characterized based on therapeutic approach and tumor pathology using Kaplan-Meier and Cox regression analyses. Results The mean age was 45.6 years (range: 19-77). Gross total resection (GTR) was achieved in 13 patients, whereas 5 patients underwent subtotal resection. Median follow-up was 91.5 months (range: 8-357). The 5-, 10-, and 15-year recurrence-free survival (RFS) rates were 61, 41, and 20%, respectively. Six patients developed metastases at an average of 113 months (range: 42-231). OS at last follow-up was 80%. Importantly, immediate postoperative adjuvant radiotherapy (IRT) did not influence RFS compared with surgery alone or OS compared with delayed radiotherapy at the time of recurrence. Conclusion HPCs have high recurrence rates necessitating close follow-up. Surgery remains an important first step, but the timing of radiotherapy for optimal control and OS remains uncertain.
Keywords: hemangiopericytoma; intracranial; radiotherapy; recurrence; survival.
Figures



References
-
- Begg C F, Garret R. Hemangiopericytoma occurring in the meninges: case report. Cancer. 1954;7(03):602–606. - PubMed
-
- Damodaran O, Robbins P, Knuckey N, Bynevelt M, Wong G, Lee G. Primary intracranial haemangiopericytoma: comparison of survival outcomes and metastatic potential in WHO grade II and III variants. J Clin Neurosci. 2014;21(08):1310–1314. - PubMed
-
- Louis D N, Ohgaki H, Wiestler O D, Cavenee W K, Ellison D W. Lyon, France: World Health Organization; 2016. WHO Classification of Tumours of the Central Nervous System. Revised Fo; p. 408.
-
- Perry A, Scheithauer B W, Nascimento A G. The immunophenotypic spectrum of meningeal hemangiopericytoma: a comparison with fibrous meningioma and solitary fibrous tumor of meninges. Am J Surg Pathol. 1997;21(11):1354–1360. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
