

Quality Improvement Intervention for Reduction of Redundant Testing
- PMID: 28725791
- PMCID: PMC5497914
- DOI: 10.1177/2374289517707506
Quality Improvement Intervention for Reduction of Redundant Testing
Abstract
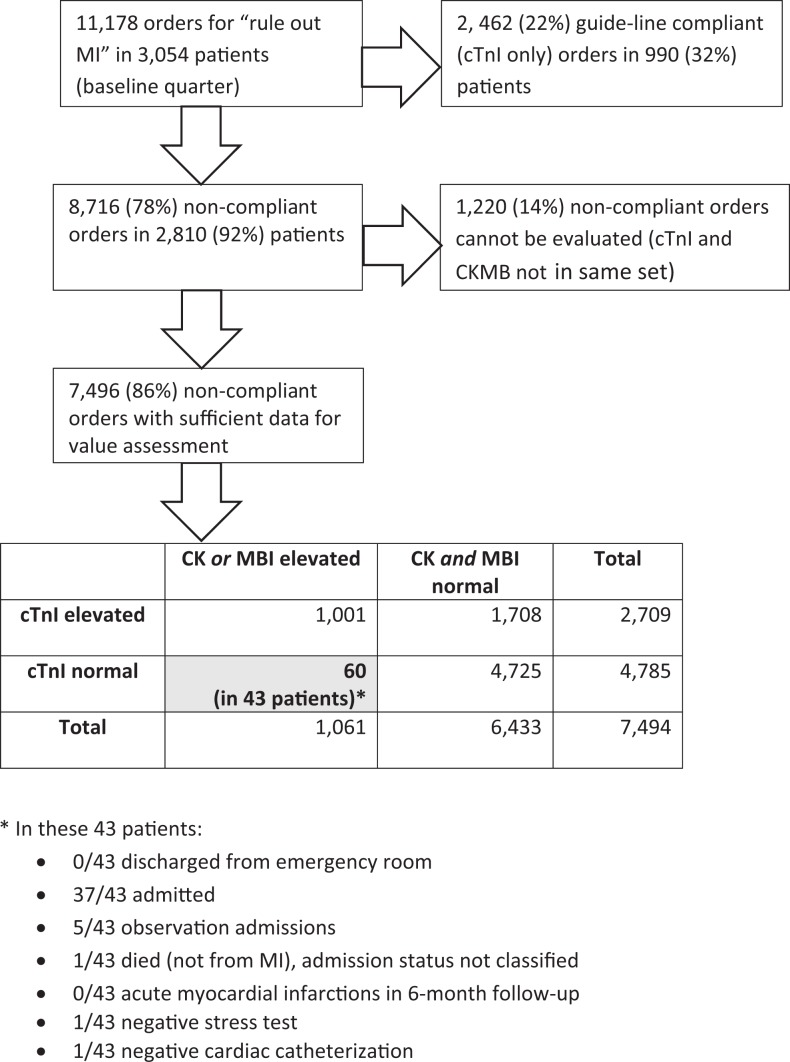
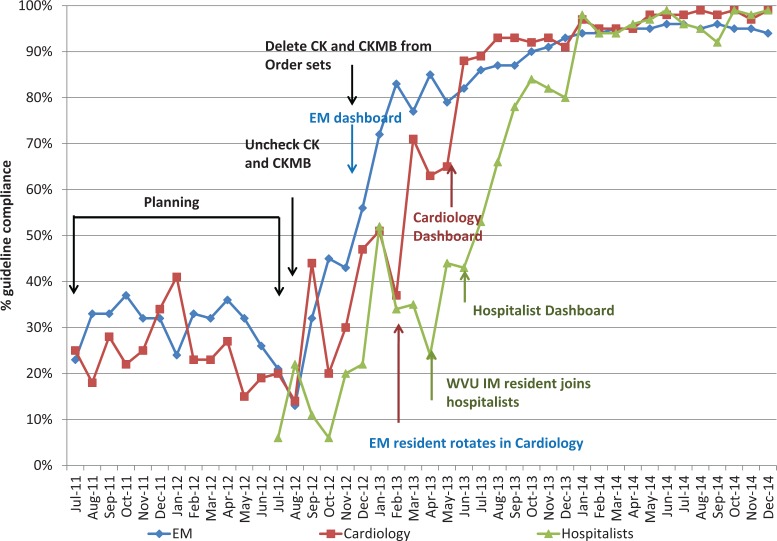
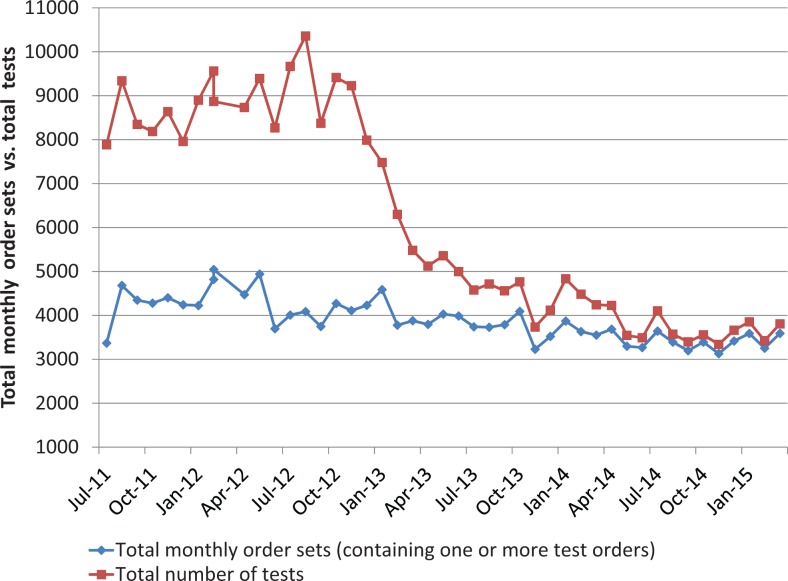
Laboratory data are critical to analyzing and improving clinical quality. In the setting of residual use of creatine kinase M and B isoenzyme testing for myocardial infarction, we assessed disease outcomes of discordant creatine kinase M and B isoenzyme +/troponin I (-) test pairs in order to address anticipated clinician concerns about potential loss of case-finding sensitivity following proposed discontinuation of routine creatine kinase and creatine kinase M and B isoenzyme testing. Time-sequenced interventions were introduced. The main outcome was the percentage of cardiac marker studies performed within guidelines. Nonguideline orders dominated at baseline. Creatine kinase M and B isoenzyme testing in 7496 order sets failed to detect additional myocardial infarctions but was associated with 42 potentially preventable admissions/quarter. Interruptive computerized soft stops improved guideline compliance from 32.3% to 58% (P < .001) in services not receiving peer leader intervention and to >80% (P < .001) with peer leadership that featured dashboard feedback about test order performance. This successful experience was recapitulated in interrupted time series within 2 additional services within facility 1 and then in 2 external hospitals (including a critical access facility). Improvements have been sustained postintervention. Laboratory cost savings at the academic facility were estimated to be ≥US$635 000 per year. National collaborative data indicated that facility 1 improved its order patterns from fourth to first quartile compared to peer norms and imply that nonguideline orders persist elsewhere. This example illustrates how pathologists can provide leadership in assisting clinicians in changing laboratory ordering practices. We found that clinicians respond to local laboratory data about their own test performance and that evidence suggesting harm is more compelling to clinicians than evidence of cost savings. Our experience indicates that interventions done at an academic facility can be readily instituted by private practitioners at external facilities. The intervention data also supplement existing literature that electronic order interruptions are more successful when combined with modalities that rely on peer education combined with dashboard feedback about laboratory order performance. The findings may have implications for the role of the pathology laboratory in the ongoing pivot from quantity-based to value-based health care.
Keywords: creatine kinase MB form; decision support techniques; interrupted time series analysis; myocardial infarction; pathologists; patient safety; quality improvement.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

References
-
- Lin GA, Redberg RF. Addressing overuse of medical services one decision at a time. JAMA Intern Med. 2015;175:1092–1093. doi:10.1001/jamainternmed.2015.1693. - PubMed
-
- Zhan C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. 2003;290:1868–1874. doi:10.1001/jama.290.14.1868. - PubMed
-
- Counts JM, Astles JR, Lipman HB. Assessing physician utilization of laboratory practice guidelines: barriers and opportunities for improvement. Clin Biochem. 2013;46:1554–1560. doi:10.1016/j.clinbiochem.2013.06.004. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
