

An Automated Inpatient Split-dose Bowel Preparation System Improves Colonoscopy Quality and Reduces Repeat Procedures
- PMID: 28727629
- PMCID: PMC5775057
- DOI: 10.1097/MCG.0000000000000849
An Automated Inpatient Split-dose Bowel Preparation System Improves Colonoscopy Quality and Reduces Repeat Procedures
Abstract
Background/goals: Inpatient colonoscopy preparations are often inadequate, compromising patient safety and procedure quality, while resulting in greater hospital costs. The aims of this study were to: (1) design and implement an electronic inpatient split-dose bowel preparation order set; (2) assess the intervention's impact upon preparation adequacy, repeated colonoscopies, hospital days, and costs.
Study: We conducted a single center prospective pragmatic quasiexperimental study of hospitalized adults undergoing colonoscopy. The experimental intervention was designed using DMAIC (define, measure, analyze, improve, and control) methodology. Prospective data collected over 12 months were compared with data from a historical preintervention cohort. The primary outcome was bowel preparation quality and secondary outcomes included number of repeated procedures, hospital days, and costs.
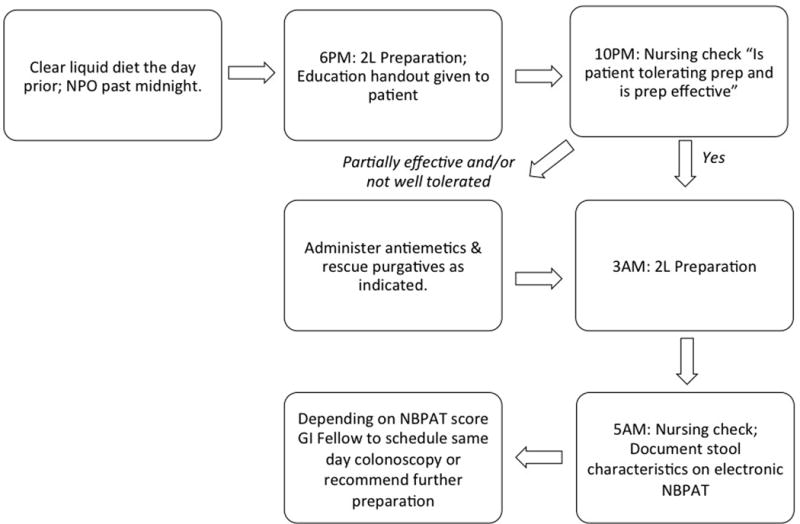
Results: On the basis of a Delphi method and DMAIC process, we created an electronic inpatient bowel preparation order set inclusive of a split-dose bowel preparation algorithm, automated orders for rescue medications, and nursing bowel preparation checks. The analysis data set included 969 patients, 445 (46%) in the postintervention group. The adequacy of bowel preparation significantly increased following intervention (86% vs. 43%; P<0.01) and proportion of repeated procedures decreased (2.0% vs. 4.6%; P=0.03). Mean hospital days from bowel preparation initiation to discharge decreased from 8.0 to 6.9 days (P=0.02). The intervention resulted in an estimated 1-year cost-savings of $46,076 based on a reduction in excess hospital days associated with repeated and delayed procedures.
Conclusions: Our interdisciplinary initiative targeting inpatient colonoscopy preparations significantly improved quality and reduced repeat procedures, and hospital days. Other institutions should consider utilizing this framework to improve inpatient colonoscopy value.
Conflict of interest statement
Figures


References
-
- Chorev N, Chadad B, Segal N, et al. Preparation for colonoscopy in hospitalized patients. Dig Dis Sci. 2007;52(3):835–9. - PubMed
-
- Reilly T, Walker G. Reasons for poor colonic preparation with inpatients. Gastroenterol Nurs. 2004;27(3):115–7. - PubMed
-
- Yadlapati R, Johnston ER, Gregory DL, et al. Predictors of Inadequate Inpatient Colonoscopy Preparation and Its Association with Hospital Length of Stay and Costs. Dig Dis Sci. 2015 - PubMed
-
- Lebwohl B, Wang TC, Neugut AI. Socioeconomic and other predictors of colonoscopy preparation quality. Dig Dis Sci. 2010;55(7):2014–20. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
