

Diagnostic accuracy of procalcitonin, neutrophil-lymphocyte count ratio, C-reactive protein, and lactate in patients with suspected bacterial sepsis
- PMID: 28727802
- PMCID: PMC5519182
- DOI: 10.1371/journal.pone.0181704
Diagnostic accuracy of procalcitonin, neutrophil-lymphocyte count ratio, C-reactive protein, and lactate in patients with suspected bacterial sepsis
Abstract
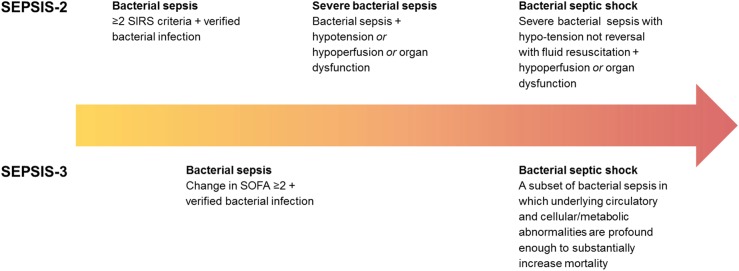
Background: Early recognition is a key factor to achieve improved outcomes for septic patients. Combinations of biomarkers, as opposed to single ones, may improve timely diagnosis and survival. We investigated the performance characteristics of sepsis biomarkers, alone and in combination, for diagnosis of verified bacterial sepsis using Sepsis-2 and Sepsis-3 criteria, respectively.
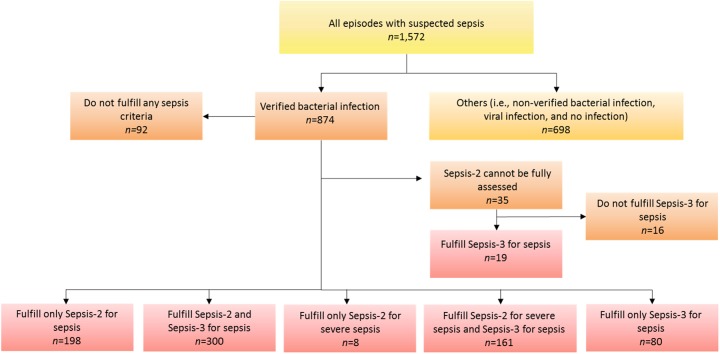
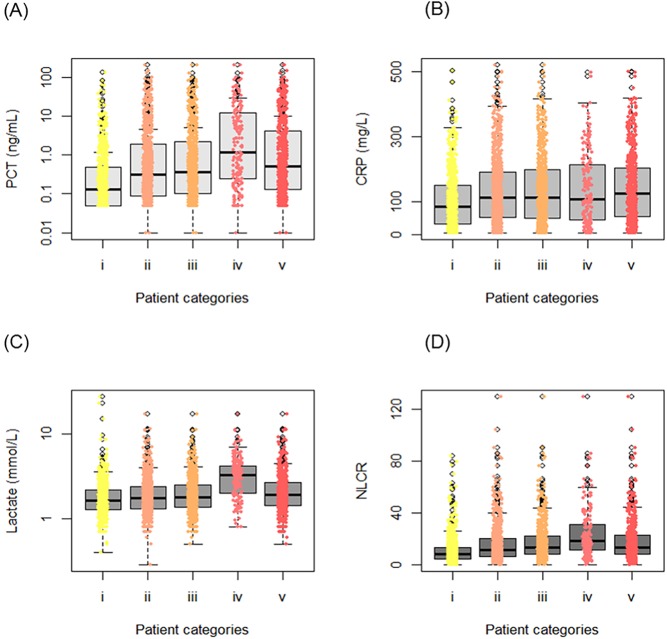
Methods: Procalcitonin (PCT), neutrophil-lymphocyte count ratio (NLCR), C-reactive protein (CRP), and lactate were determined in a total of 1,572 episodes of adult patients admitted to the emergency department on suspicion of sepsis. All sampling were performed prior to antibiotic administration. Discriminant analysis was used to construct two composite biomarkers consisting of linear combinations of the investigated biomarkers, one including three selected biomarkers (i.e., NLCR, CRP, and lactate), and another including all four (i.e., PCT, NLCR, CRP, and lactate). The diagnostic performances of the composite biomarkers as well as the individual biomarkers were compared using the area under the receiver operating characteristic curve (AUC).
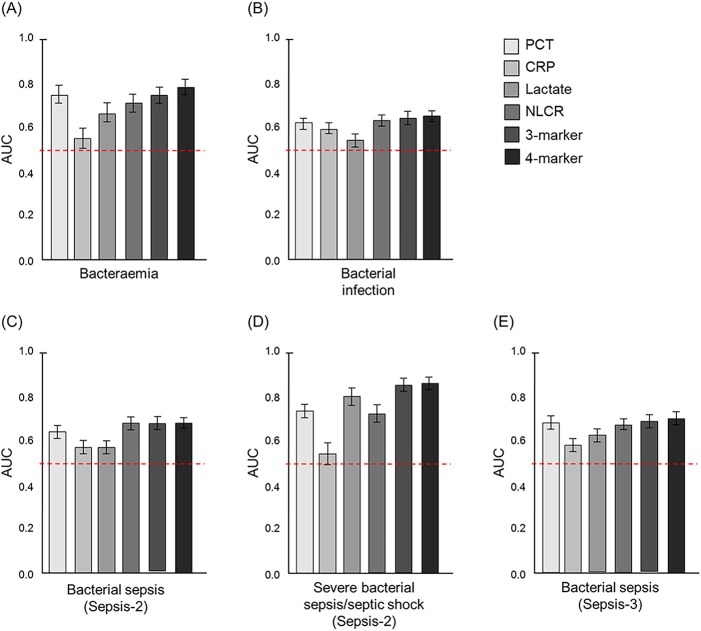
Results: For diagnosis of bacterial sepsis based on Sepsis-3 criteria, the AUC for PCT (0.68; 95% CI 0.65-0.71) was comparable to the AUCs for the both composite biomarkers. Using the Sepsis-2 criteria for bacterial sepsis diagnosis, the AUC for the NLCR (0.68; 95% CI 0.65-0.71) but not for the other single biomarkers, was equal to the AUCs for the both composite biomarkers. For diagnosis of severe bacterial sepsis or septic shock based on the Sepsis-2 criteria, the AUCs for both composite biomarkers were significantly greater than those of the single biomarkers (0.85; 95% CI 0.82-0.88 for the composite three-biomarker, and 0.86; 95% CI 0.83-0.89 for the composite four-biomarker).
Conclusions: Combinations of biomarkers can improve the diagnosis of verified bacterial sepsis in the most critically ill patients, but in less severe septic conditions either the NLCR or PCT alone exhibit equivalent performance.
Conflict of interest statement
Figures
References
-
- Singer M, Deutschman CS, Seymour CW, Shankar-Hari M, Annane D, Bauer M, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). Jama. 2016;315(8):801–10. Epub 2016/02/24. doi: 10.1001/jama.2016.0287 ; PubMed Central PMCID: PMCPMC4968574. - DOI - PMC - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. 2013;39(2):165–228. Epub 2013/01/31. doi: 10.1007/s00134-012-2769-8 . - DOI - PMC - PubMed
-
- Kumar A, Ellis P, Arabi Y, Roberts D, Light B, Parrillo JE, et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest. 2009;136(5):1237–48. Epub 2009/08/22. doi: 10.1378/chest.09-0087 . - DOI - PubMed
-
- Seymour CW, Gesten F, Prescott HC, Friedrich ME, Iwashyna TJ, Phillips GS, et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N Engl J Med. 2017;376(23):2235–44. Epub 2017/05/23. doi: 10.1056/NEJMoa1703058 . - DOI - PMC - PubMed
-
- Craig JC, Williams GJ, Jones M, Codarini M, Macaskill P, Hayen A, et al. The accuracy of clinical symptoms and signs for the diagnosis of serious bacterial infection in young febrile children: prospective cohort study of 15 781 febrile illnesses. Bmj. 2010;340:c1594 Epub 2010/04/22. doi: 10.1136/bmj.c1594 ; PubMed Central PMCID: PMCPmc2857748. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
