

Proton Beam Radiotherapy and Concurrent Chemotherapy for Unresectable Stage III Non-Small Cell Lung Cancer: Final Results of a Phase 2 Study
- PMID: 28727865
- PMCID: PMC5824219
- DOI: 10.1001/jamaoncol.2017.2032
Proton Beam Radiotherapy and Concurrent Chemotherapy for Unresectable Stage III Non-Small Cell Lung Cancer: Final Results of a Phase 2 Study
Erratum in
-
Error in Figure.JAMA Oncol. 2017 Sep 1;3(9):1286. doi: 10.1001/jamaoncol.2017.3416. JAMA Oncol. 2017. PMID: 28910457 Free PMC article. No abstract available.
-
Error in Kaplan-Meier Curves.JAMA Oncol. 2017 Dec 1;3(12):1742. doi: 10.1001/jamaoncol.2017.4131. JAMA Oncol. 2017. PMID: 29075774 Free PMC article. No abstract available.
Abstract
Importance: Proton beam radiotherapy (PBT) has the potential to reduce toxic effects in the definitive management of locally advanced non-small cell lung cancer (NSCLC), but long-term prospective data are lacking.
Objective: To report the final (5-year) results of a prospective study evaluating concurrent chemotherapy and high-dose PBT to treat unresectable stage III NSCLC.
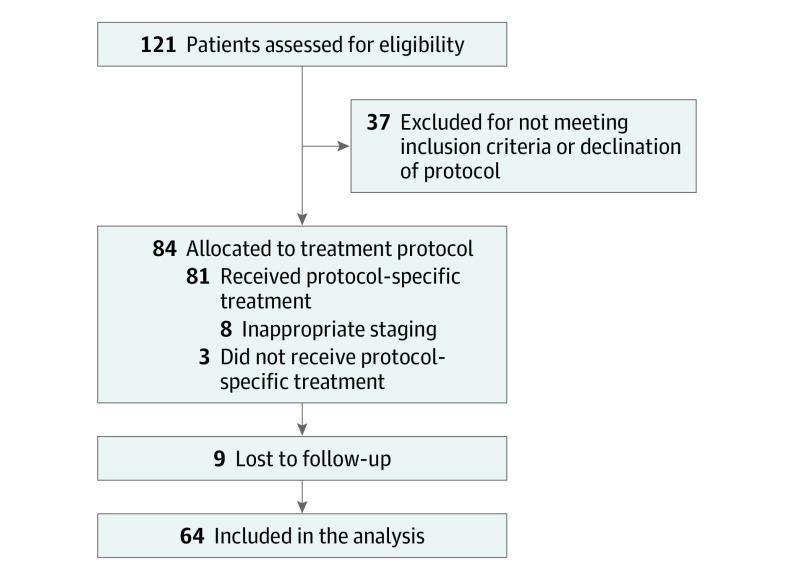
Design, setting, and participants: In this open-label, single-group assignment study, with median follow-up of 27.3 months for all patients and 79.6 months for survivors, 64 patients were enrolled and analyzed; inclusion criteria were unresectable IIIA/IIIB histologically confirmed NSCLC, Karnofsky performance status 70 to 100, and 6-month prediagnosis weight loss of no more than 10%. Staging used positron emission tomography and/or computed tomography. Induction chemotherapy was allowed.
Interventions: Concurrent chemotherapy (carboplatin-paclitaxel) and passively scattered PBT (74-Gy relative biological effectiveness) in all patients.
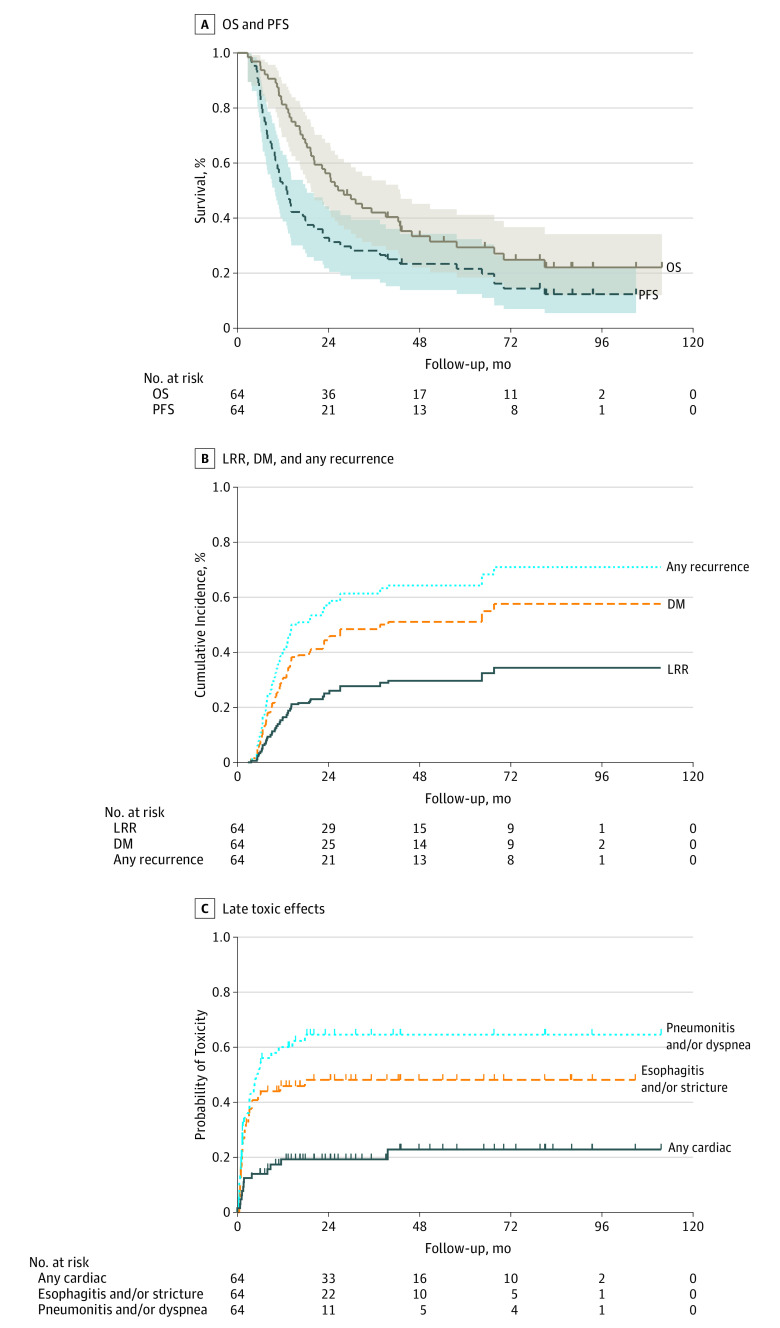
Main outcomes and measures: Kaplan-Meier analysis of overall survival (OS), progression-free survival (PFS), actuarial distant metastasis, and locoregional recurrence. Patterns of treatment failure were categorized as local/regional or distant. Acute and late toxic effects were prospectively assigned using Common Terminology Criteria for Adverse Events, v3.0.
Results: Of 64 patients (22 [34%] female; median [range] age, 70 [37-78] years; stage IIIA, 30 [47%]; IIIB, 34 [53%]), 17 (27%) were alive at last follow-up. Median OS was 26.5 months (5-year OS, 29%; 95% CI, 18%-41%). Five-year PFS was 22% (95% CI, 12%-32%); 5-year actuarial distant metastasis and locoregional recurrence were 54% (n = 36) and 28% (n = 22), respectively. Treatment failures were largely (31 [48%] patients) distant, with low rates of crude local (10 [16%]) and regional (9 [14%]) recurrences. Rates of grade 2 and 3 acute esophagitis were 18 (28%) and 5 (8%), respectively. Acute grade 2 pneumonitis occurred in 1 (2%) patient. Late toxic effects were uncommon: 1 (2%) patient developed an esophageal stricture (grade 2) and 1 (2%) grade 4 esophagitis. Late grades 2 and 3 pneumonitis occurred in 10 (16%) and 8 (12%), respectively. Two (3%) patients developed a bronchial stricture (grade 2), and 1 (2%) a grade 4 bronchial fistula. There were no acute or late grade 5 toxic effects.
Conclusions and relevance: Concurrent chemotherapy and PBT to treat unresectable NSCLC afford promising clinical outcomes and rates of toxic effects compared with historical photon therapy data. Further optimization of proton therapy, particularly intensity-modulated proton therapy, is still needed.
Conflict of interest statement
Figures
Comment in
-
Breaking the dose ceiling: proton therapy for locally advanced non-small cell lung cancer.J Thorac Dis. 2018 Jan;10(1):130-134. doi: 10.21037/jtd.2017.12.79. J Thorac Dis. 2018. PMID: 29600039 Free PMC article. No abstract available.
-
Stage III non-small cell lung cancer: escalation matters, but how?Transl Lung Cancer Res. 2018 Apr;7(Suppl 2):S107-S110. doi: 10.21037/tlcr.2018.03.02. Transl Lung Cancer Res. 2018. PMID: 29780703 Free PMC article. No abstract available.
References
-
- National Comprehensive Cancer Network . Non-Small Cell Lung Cancer. Version 1.2016. https://www.nccn.org/professionals/physician_gls/PDF/nsclc.pdf. Accessed January 2, 2017.
-
- Chang JY, Zhang X, Wang X, et al. . Significant reduction of normal tissue dose by proton radiotherapy compared with three-dimensional conformal or intensity-modulated radiation therapy in stage I or stage III non-small-cell lung cancer. Int J Radiat Oncol Biol Phys. 2006;65(4):1087-1096. - PubMed
-
- Sejpal S, Komaki R, Tsao A, et al. . Early findings on toxicity of proton beam therapy with concurrent chemotherapy for nonsmall cell lung cancer. Cancer. 2011;117(13):3004-3013. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
