

Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular hemorrhage in preterm infants
- PMID: 28727900
- PMCID: PMC6483558
- DOI: 10.1002/14651858.CD012362.pub2
Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular hemorrhage in preterm infants
Update in
-
Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular haemorrhage in preterm infants.Cochrane Database Syst Rev. 2020 Jul 7;7(7):CD012362. doi: 10.1002/14651858.CD012362.pub3. Cochrane Database Syst Rev. 2020. PMID: 32639053 Free PMC article.
Abstract
Background: Preterm birth is known to constitute the major risk factor for development of germinal matrix-intraventricular hemorrhage (GM-IVH). Head position may affect cerebral hemodynamics and thus may be involved indirectly in development of GM-IVH. Turning the head toward one side may functionally occlude jugular venous drainage on the ipsilateral side while increasing intracranial pressure and cerebral blood volume. Thus, it has been suggested that cerebral venous pressure is reduced and hydrostatic brain drainage improved if the patient is in supine midline position with the bed tilted 30°. The midline position might be achieved in the supine position and, with the use of physical aids, in the lateral position as well. Midline position should be kept, at least when the incidence of GM-IVH is greatest, that is, during the first two to three days of life.
Objectives: Primary objective To assess whether head midline position is more effective than any other head position for preventing or extending germinal matrix-intraventricular hemorrhage in infants born at ≤ 32 weeks' gestational age. Secondary objectives To perform subgroup analyses regarding gestational age, birth weight, intubated versus not intubated, and with or without GM-IVH at trial entry.
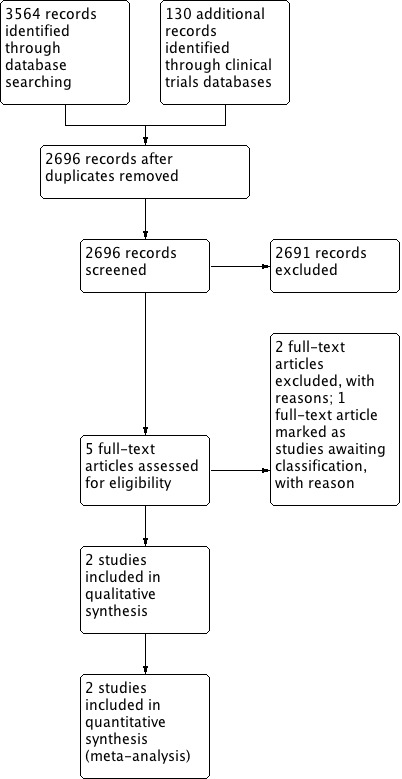
Search methods: We used the standard search strategy of the Cochrane Neonatal Review Group to search the Cochrane Central Register of Controlled Trials (CENTRAL; 2016, Issue 8), MEDLINE via PubMed (1966 to September 19, 2016), Embase (1980 to September 19,.2016), and the Cumulative Index to Nursing and Allied Health Literature (CINAHL; 1982 to September 19, 2016). We searched clinical trials databases, conference proceedings, and reference lists of retrieved articles for randomized controlled trials and quasi-randomized trials.
Selection criteria: Randomized clinical controlled trials, quasi-randomized trials, and cluster-randomized controlled trials comparing placing very preterm infants in a head midline position versus placing them in a prone or lateral decubitus position, or undertaking a strategy of regular position change, or having no prespecified position. We included trials enrolling infants with existing GM-IVH and planned to assess extension of hemorrhage in a subgroup of infants. We planned to analyze horizontal (flat) versus head elevated positions separately for all body positions.
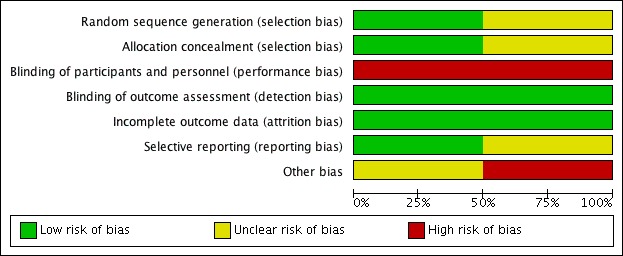
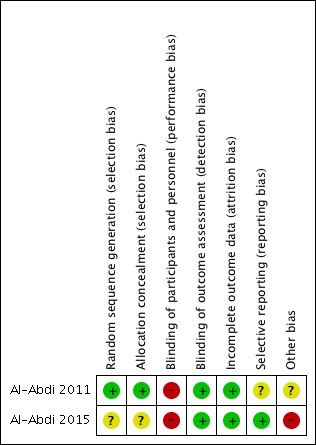
Data collection and analysis: We used standard methods of the Cochrane Neonatal Review Group. For each of the included trials, two review authors independently extracted data (e.g., number of participants, birth weight, gestational age, initiation and duration of head midline position, co-intervention with horizontal vs head elevated position, use of physical aids to maintain head position) and assessed risk of bias (e.g., adequacy of randomization, blinding, completeness of follow-up). The primary outcomes considered in this review are GM-IVH , severe IVH, and neonatal death.
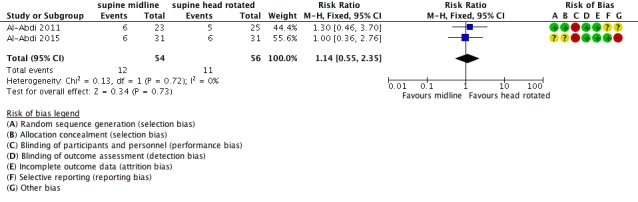
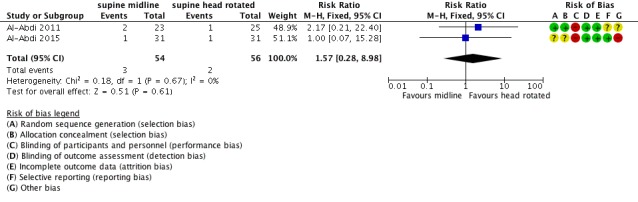
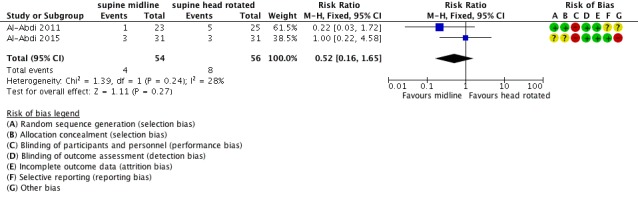
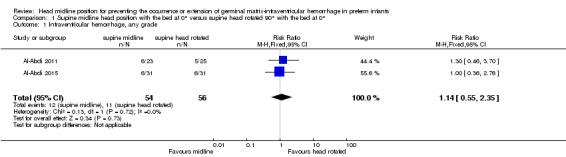
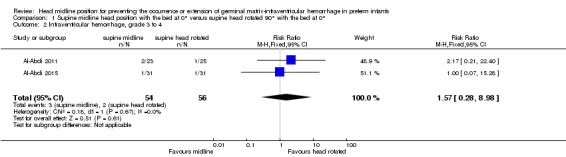
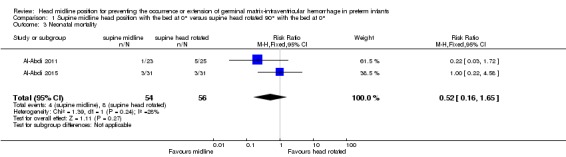
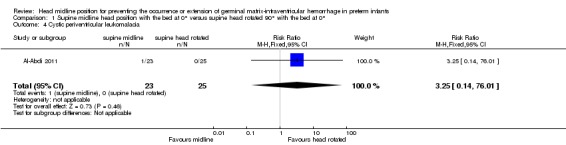
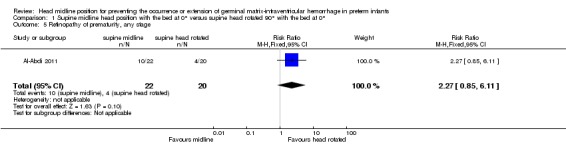
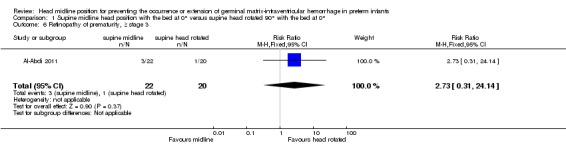
Main results: Our search strategy yielded 2696 references. Two review authors independently assessed all references for inclusion. Two randomized controlled trials, for a total of 110 infants, met the inclusion criteria of this review. Both trials compared supine midline head position with the bed at 0° versus supine head rotated 90° with the bed at 0°. We found no trials that compared supine versus prone midline head position, and no trials that compared effects of head tilting. We found no significant differences in rates of GM-IVH (typical risk ratio [RR] 1.14, 95% confidence interval [CI] 0.55 to 2.35; typical risk difference [RD] 0.03, 95% CI -0.13 to 0.18; two studies, 110 infants; I2 = 0% for RR and I2 = 0% for RD), severe IVH (typical RR 1.57, 95% CI 0.28 to 8.98; typical RD 0.02, 95% CI -0.06 to 0.10; two studies, 110 infants; I2 = 0% for RR and I2 = 0% for RD), and neonatal mortality (typical RR 0.52, 95% CI 0.16 to 1.65; typical RD -0.07, 95% CI -0.18 to 0.05; two studies, 110 infants; I2 = 28% for RR and I2 = 44% for RD). Among secondary outcomes, we found no significant differences in terms of cystic periventricular leukomalacia (one study; RR 3.25, 95% CI 0.14 to 76.01; RD 0.04, 95% CI -0.07 to 0.15), retinopathy of prematurity (one study; RR 2.27, 95% CI 0.85 to 6.11; RD 0.25, 95% CI -0.02 to 0.53), and severe retinopathy of prematurity (one study; RR 2.73, 95% CI 0.31 to 24.14; RD 0.09, 95% CI -0.09 to 0.26). None of the included trials reported on the other specified outcomes of this review (i.e., cerebellar hemorrhage, brain magnetic resonance imaging abnormalities, impairment in cerebral hemodynamics, long-term neurodevelopmental outcomes, and major neurodevelopmental disability). The quality of evidence supporting these findings is limited owing to the imprecision of the estimates. We identified no ongoing studies.
Authors' conclusions: Given the imprecision of the estimate, results of this systematic review are consistent with beneficial or detrimental effects of a supine head midline position versus a lateral position and do not provide a definitive answer to the review question.
Conflict of interest statement
OR, MGC, and MB have no known conflicts of interest to declare.
Figures
Similar articles
-
Head midline position for preventing the occurrence or extension of germinal matrix-intraventricular haemorrhage in preterm infants.Cochrane Database Syst Rev. 2020 Jul 7;7(7):CD012362. doi: 10.1002/14651858.CD012362.pub3. Cochrane Database Syst Rev. 2020. PMID: 32639053 Free PMC article.
-
Heparin for the prevention of intraventricular haemorrhage in preterm infants.Cochrane Database Syst Rev. 2016 May 5;2016(5):CD011718. doi: 10.1002/14651858.CD011718.pub2. Cochrane Database Syst Rev. 2016. PMID: 27148674 Free PMC article.
-
Antithrombin for the prevention of intraventricular hemorrhage in very preterm infants.Cochrane Database Syst Rev. 2016 Mar 21;3:CD011636. doi: 10.1002/14651858.CD011636.pub2. Cochrane Database Syst Rev. 2016. PMID: 26998583
-
Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants.Cochrane Database Syst Rev. 2017 Apr 11;4(4):CD011190. doi: 10.1002/14651858.CD011190.pub2. Cochrane Database Syst Rev. 2017. PMID: 28398697 Free PMC article.
-
Early erythropoiesis-stimulating agents in preterm or low birth weight infants.Cochrane Database Syst Rev. 2017 Nov 16;11(11):CD004863. doi: 10.1002/14651858.CD004863.pub5. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Feb 11;2:CD004863. doi: 10.1002/14651858.CD004863.pub6. PMID: 29145693 Free PMC article. Updated.
Cited by
-
Impact of a "Brain Protection Bundle" in Reducing Severe Intraventricular Hemorrhage in Preterm Infants <30 Weeks GA: A Retrospective Single Centre Study.Children (Basel). 2021 Oct 31;8(11):983. doi: 10.3390/children8110983. Children (Basel). 2021. PMID: 34828696 Free PMC article.
-
Germinal Matrix-Intraventricular Hemorrhage: A Tale of Preterm Infants.Int J Pediatr. 2021 Mar 16;2021:6622598. doi: 10.1155/2021/6622598. eCollection 2021. Int J Pediatr. 2021. PMID: 33815512 Free PMC article. Review.
-
Prevention, Reduction and Repair of Brain Injury of the Preterm Infant.Front Physiol. 2019 Mar 20;10:181. doi: 10.3389/fphys.2019.00181. eCollection 2019. Front Physiol. 2019. PMID: 30949060 Free PMC article. Review.
-
Respiratory Care for the Ventilated Neonate.Can Respir J. 2018 Aug 13;2018:7472964. doi: 10.1155/2018/7472964. eCollection 2018. Can Respir J. 2018. PMID: 30186538 Free PMC article. Review.
-
Neuroprotection from acute brain injury in preterm infants.Paediatr Child Health. 2019 Jul;24(4):276-290. doi: 10.1093/pch/pxz056. Epub 2019 Jun 21. Paediatr Child Health. 2019. PMID: 31239818 Free PMC article. Review.
References
References to studies included in this review
-
- Al‐Abdi SY, Nojoom MS, Alshaalan HM, Al‐Aamri MA. Pilot‐randomized study on intraventricular hemorrhage with midline versus lateral head positions. Saudi Medical Journal 2011;32(4):420‐1. - PubMed
-
- Al‐Abdi S, Alallah J, Al Omran A, Al Alwan Q, Al Hashimi H, Haidar S. The risk of intraventricular hemorrhage with flat midline versus flat right lateral head positions: a prematurely terminated multicenter randomized clinical trial. The Pediatric Academic Societies (PAS). 2015. [https://clinicaltrials.gov/ct2/show/NCT01584375]
References to studies excluded from this review
-
- Antunes LC, Rugolo LM, Crocci AJ. Effect of preterm infant position on weaning from mechanical ventilation [Efeito da posição do prematuro no desmame da ventilação mecânica]. Jornal de Pediatria 2003;79(3):239‐44. - PubMed
-
- Wu J, Zhai J, Jiang H, Sun Y, Jin B, Zhang Y, et al. Effect of change of mechanical ventilation position on the treatment of neonatal respiratory failure. Cell Biochemistry and Biophysics 2015;72(3):845‐9. - PubMed
References to studies awaiting assessment
Additional references
-
- Bayley N. Bayley Scales of Infant Development. 2nd Edition. San Antonio, TX: The Psychological Corporation, 1993.
-
- Bayley N. Bayley Scales of Infant and Toddler Development. 3rd Edition. San Antonio, TX: Harcourt Assessment, 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous