

Birth weight differences between those offered financial voucher incentives for verified smoking cessation and control participants enrolled in the Cessation in Pregnancy Incentives Trial (CPIT), employing an intuitive approach and a Complier Average Causal Effects (CACE) analysis
- PMID: 28728583
- PMCID: PMC5520300
- DOI: 10.1186/s13063-017-2053-x
Birth weight differences between those offered financial voucher incentives for verified smoking cessation and control participants enrolled in the Cessation in Pregnancy Incentives Trial (CPIT), employing an intuitive approach and a Complier Average Causal Effects (CACE) analysis
Abstract
Background: The Cessation in Pregnancy Incentives Trial (CPIT), which offered financial incentives for smoking cessation during pregnancy showed a clinically and statistically significant improvement in cessation. However, infant birth weight was not seen to be affected. This study re-examines birth weight using an intuitive and a complier average causal effects (CACE) method to uncover important information missed by intention-to-treat analysis.
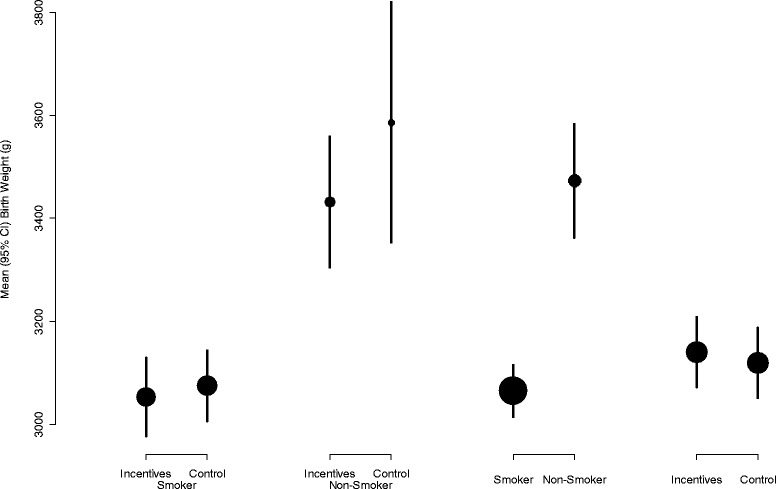
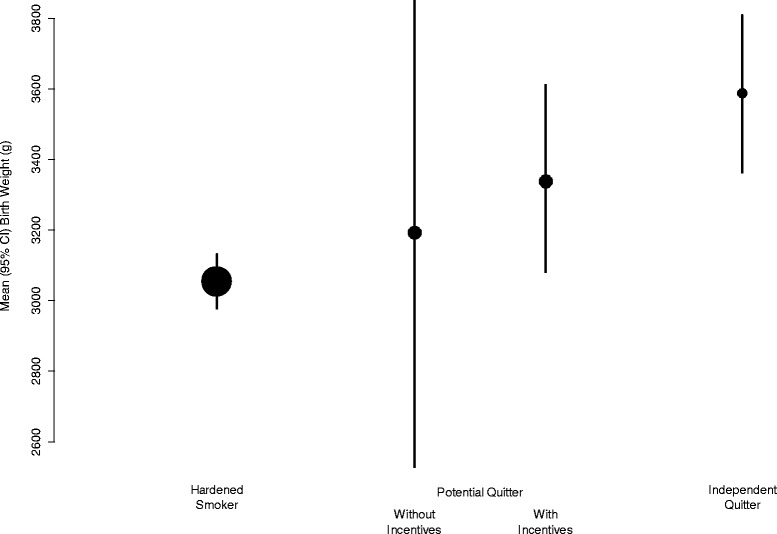
Methods: CPIT offered financial incentives up to £400 to pregnant smokers to quit. With incentives, 68 women (23.1%) were confirmed non-smokers at primary outcome, compared to 25 (8.7%) without incentives, a difference of 14.3% (Fisher test, p < 0.0001). For this analysis, randomised groups were split into three theoretical sub-groups: independent quitters - quit without incentives, hardened smokers - could not quit even with incentives and potential quitters - required the addition of financial incentives to quit. Viewed in this way, the overall birth weight gain with incentives is attributable only to potential quitters. We compared an intuitive approach to a CACE analysis.
Results: Mean birth weight of potential quitters in the incentives intervention group (who therefore quit) was 3338 g compared with potential quitters in the control group (who did not quit) 3193 g. The difference attributable to incentives, was 3338 - 3193 = 145 g (95% CI -617, +803). The mean difference in birth weight between the intervention and control groups was 21 g, and the difference in the proportion who managed to quit was 14.3%. Since the intervention consisted of the offer of incentives to quit smoking, the intervention was received by all women in the intervention group. However, "compliance" was successfully quitting with incentives, and the CACE analysis yielded an identical result, causal birth weight increase 21 g ÷ 0.143 = 145 g.
Conclusions: Policy makers have great difficulty giving pregnant women money to stop smoking. This study indicates that a small clinically insignificant improvement in average birth weight is likely to hide an important clinically significant increase in infants born to pregnant smokers who want to stop but cannot achieve smoking cessation without the addition of financial voucher incentives.
Trial registration: ISRCTN Registry, ISRCTN87508788 . Registered on 1 September 2011.
Keywords: Birth weight; Pregnancy; Smoking cessation; Treatment effectiveness.
Conflict of interest statement
Authors’ information
1. Alex McConnachie is Deputy Director of the Robertson Centre for Biostatistics, Glasgow University.
2. Caroline Haig is a Post Doctoral Statistician in the Robertson Centre for Biostatistics, Glasgow University.
3. Linda Bauld (Co-Principal Investigator) is Professor of Health Policy, University of Stirling and UK Centre for Tobacco and Alcohol Studies, and has extensive experience of quantitative work related to smoking cessation.
4. Lesley Sinclair (Trial Manager) has experience of data management and the management of clinical trials.
5. David Tappin (Co-Principal Investigator) is Professor of Clinical Trials for Children based at Glasgow University.
Ethics approval and consent to participate
The Cessation in Pregnancy Incentives Trial (CPIT) was approved by the NHS West of Scotland Research Ethics Committee 2 (11/AL/0204). All participants gave informed consent to take part in this trial.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Oster G, Delea TE, Colditz GA. Maternal smoking during pregnancy and expenditures on neonatal health care. Am J Prev Med. 1988;4(4):216–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
