

Retroperitoneal Lymphadenectomy for High Risk, Nonmetastatic Renal Cell Carcinoma: An Analysis of the ASSURE (ECOG-ACRIN 2805) Adjuvant Trial
- PMID: 28728992
- PMCID: PMC5800986
- DOI: 10.1016/j.juro.2017.07.042
Retroperitoneal Lymphadenectomy for High Risk, Nonmetastatic Renal Cell Carcinoma: An Analysis of the ASSURE (ECOG-ACRIN 2805) Adjuvant Trial
Abstract
Purpose: Lymphadenectomy is a well established practice for many urological malignancies but its role in renal cell carcinoma is less clear. Our primary objective was to determine whether lymphadenectomy impacted survival in patients with fully resected, high risk renal cell carcinoma.
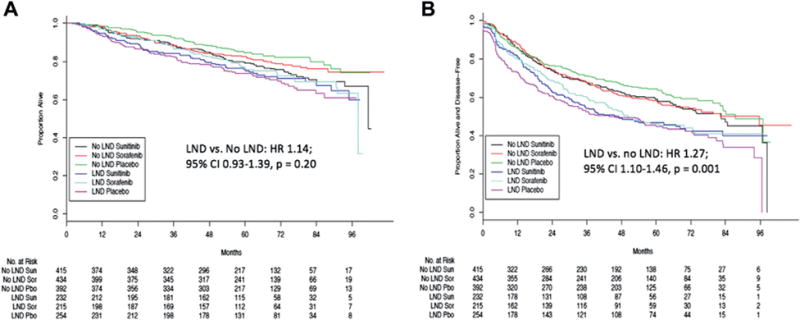
Materials and methods: Patients with fully resected, high risk, nonmetastatic renal cell carcinoma were randomized to adjuvant sorafenib, sunitinib or placebo in the ASSURE (Adjuvant Sorafenib and Sunitinib for Unfavorable Renal Carcinoma) trial. Lymphadenectomy was performed for cN+ disease or at surgeon discretion. Patients treated with lymphadenectomy were compared to patients in the trial who did not undergo lymphadenectomy. The primary outcome was overall survival associated with lymphadenectomy. Secondary outcomes were disease free survival, factors associated with performing lymphadenectomy and surgical complications.
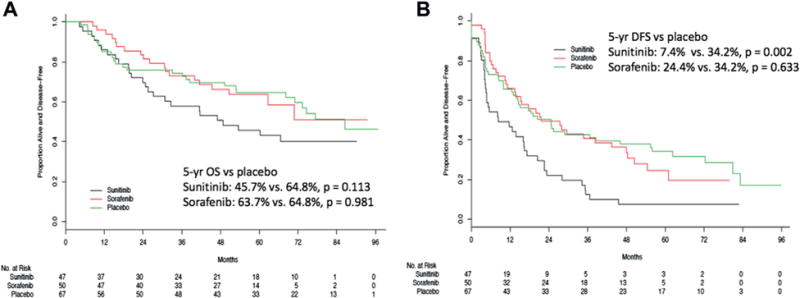
Results: Of the 1,943 patients in ASSURE 701 (36.1%) underwent lymphadenectomy, including all resectable patients with cN+ and 30.1% of those with cN0 disease. A median of 3 lymph nodes (IQR 1-8) were removed and the rate of pN+ disease in the lymphadenectomy group was 23.4%. There was no overall survival benefit for lymphadenectomy relative to no lymphadenectomy (HR 1.14, 95% CI 0.93-1.39, p = 0.20). In patients with pN+ disease who underwent lymphadenectomy no improvement in overall or disease-free survival was observed for adjuvant therapy relative to placebo. Lymphadenectomy did not confer an increased risk of surgical complications (14.2% vs 13.4%, p = 0.63).
Conclusions: The benefit of lymphadenectomy in patients undergoing surgery for high risk renal cell carcinoma remains uncertain. Future strategies to answer this question should include a prospective trial in which patients with high risk renal cell carcinoma are randomized to specific lymphadenectomy templates.
Keywords: adjuvant; carcinoma; chemotherapy; kidney; lymph node excision; mortality; renal cell.
Copyright © 2018 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Editorial Comment.J Urol. 2018 Jan;199(1):59. doi: 10.1016/j.juro.2017.07.111. Epub 2017 Oct 13. J Urol. 2018. PMID: 29031672 No abstract available.
References
-
- Mohler JL, Armstrong AJ, Bahnson RR, et al. Prostate cancer, version 1.2016. J Natl Compr Canc Netw. 2016;14:19. - PubMed
-
- Witjes JA, Comperat E, Cowan NC, et al. EAU guidelines on muscle-invasive and metastatic bladder cancer: summary of the 2013 guidelines. Eur Urol. 2014;65:778. - PubMed
-
- Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 3.2015. J Natl Compr Canc Netw. 2015;13:151. - PubMed
-
- Ljungberg B, Bensalah K, Canfield S, et al. EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol. 2015;67:913. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
