

3D Pseudocontinuous Arterial Spin-Labeling MR Imaging in the Preoperative Evaluation of Gliomas
- PMID: 28729293
- PMCID: PMC7963629
- DOI: 10.3174/ajnr.A5299
3D Pseudocontinuous Arterial Spin-Labeling MR Imaging in the Preoperative Evaluation of Gliomas
Abstract
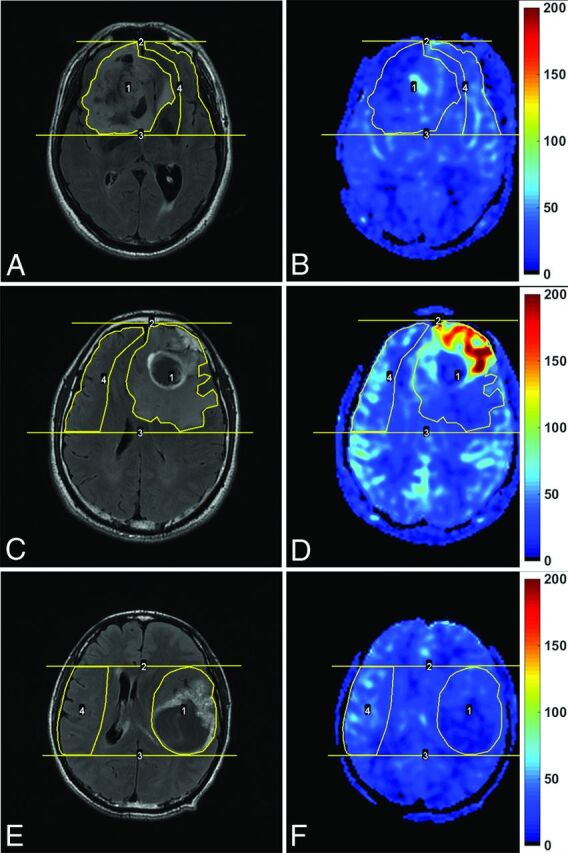
Background and purpose: Previous studies showed conflicting results concerning the value of CBF maps obtained from arterial spin-labeling MR imaging in grading gliomas. This study was performed to investigate the effectiveness of CBF maps derived from 3D pseudocontinuous arterial spin-labeling in preoperatively assessing the grade, cellular proliferation, and prognosis of gliomas.
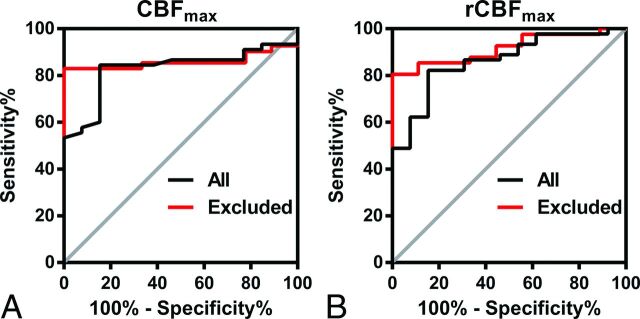
Materials and methods: Fifty-eight patients with pathologically confirmed gliomas underwent preoperative 3D pseudocontinuous arterial spin-labeling. The receiver operating characteristic curves for parameters to distinguish high-grade gliomas from low-grade gliomas were generated. Pearson correlation analysis was used to assess the correlation among parameters. Survival analysis was conducted with Cox regression.
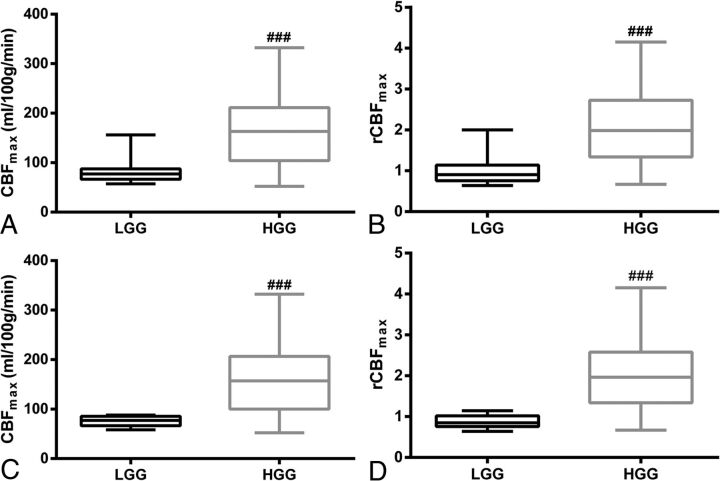
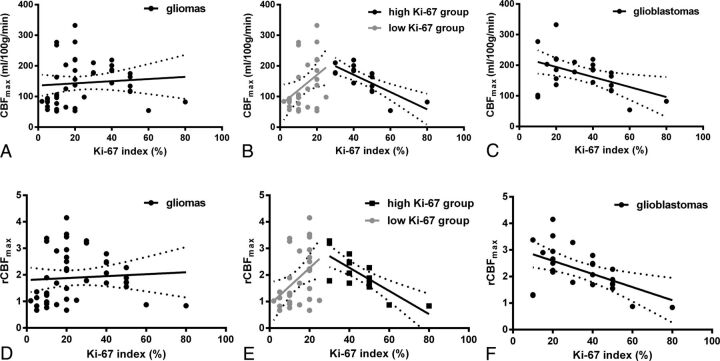
Results: Both maximum CBF and maximum relative CBF were significantly higher in high-grade gliomas than in low-grade gliomas (P < .001). The areas under the curve for maximum CBF and maximum relative CBF in distinguishing high-grade gliomas from low-grade gliomas were 0.828 and 0.863, respectively. Both maximum CBF and maximum relative CBF had no correlation with the Ki-67 index in all subjects and had a moderate negative correlation with the Ki-67 index in glioblastomas (r = -0.475, -0.534, respectively). After adjustment for age, a higher maximum CBF (P = .008) and higher maximum relative CBF (P = .005) were associated with worse progression-free survival in gliomas, while a higher maximum relative CBF (P = .033) was associated with better overall survival in glioblastomas.
Conclusions: 3D pseudocontinuous arterial spin-labeling-derived CBF maps are effective in preoperative evaluation of gliomas. Although gliomas with a higher blood flow are more malignant, glioblastomas with a lower blood flow are likely to be more aggressive.
© 2017 by American Journal of Neuroradiology.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical