

Structure of general-population antibody titer distributions to influenza A virus
- PMID: 28729702
- PMCID: PMC5519701
- DOI: 10.1038/s41598-017-06177-0
Structure of general-population antibody titer distributions to influenza A virus
Abstract
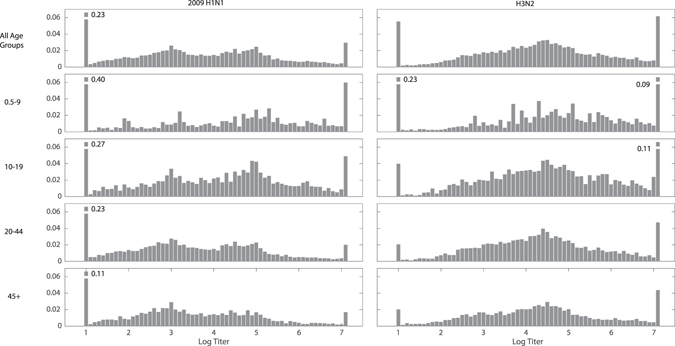
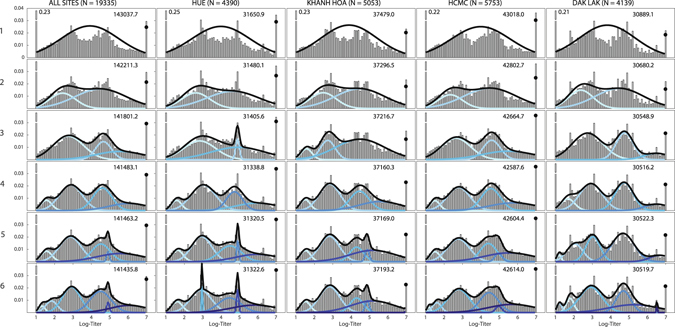
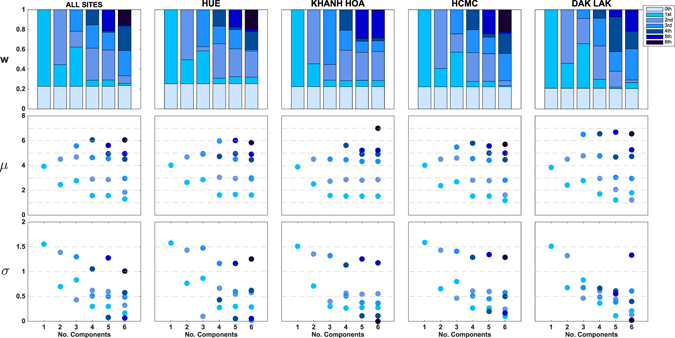
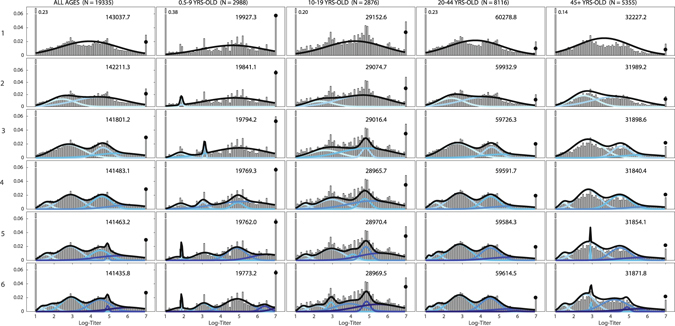
Seroepidemiological studies aim to understand population-level exposure and immunity to infectious diseases. Their results are normally presented as binary outcomes describing the presence or absence of pathogen-specific antibody, despite the fact that many assays measure continuous quantities. A population's natural distribution of antibody titers to an endemic infectious disease may include information on multiple serological states - naiveté, recent infection, non-recent infection, childhood infection - depending on the disease in question and the acquisition and waning patterns of immunity. In this study, we investigate 20,152 general-population serum samples from southern Vietnam collected between 2009 and 2013 from which we report antibody titers to the influenza virus HA1 protein using a continuous titer measurement from a protein microarray assay. We describe the distributions of antibody titers to subtypes 2009 H1N1 and H3N2. Using a model selection approach to fit mixture distributions, we show that 2009 H1N1 antibody titers fall into four titer subgroups and that H3N2 titers fall into three subgroups. For H1N1, our interpretation is that the two highest-titer subgroups correspond to recent and historical infection, which is consistent with 2009 pandemic attack rates. Similar interpretations are available for H3N2, but right-censoring of titers makes these interpretations difficult to validate.
Conflict of interest statement
MFB has been a paid consultant to Visterra Inc in Cambridge MA.
Figures
References
-
- Todd, S. Influenza in Vietnam: cross immunity from prior infection and its effect on population-level estimates of infection. (University of Liverpool and Liverpool School of Tropical Medicine, PhD Thesis, 2016).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
