

Effects of collimator angle, couch angle, and starting phase on motion-tracking dynamic conformal arc therapy (4D DCAT)
- PMID: 28730652
- PMCID: PMC5874990
- DOI: 10.1002/acm2.12132
Effects of collimator angle, couch angle, and starting phase on motion-tracking dynamic conformal arc therapy (4D DCAT)
Abstract
Purpose: The aim of this study was to find an optimized configuration of collimator angle, couch angle, and starting tracking phase to improve the delivery performance in terms of MLC position errors, maximal MLC leaf speed, and total beam-on time of DCAT plans with motion tracking (4D DCAT).
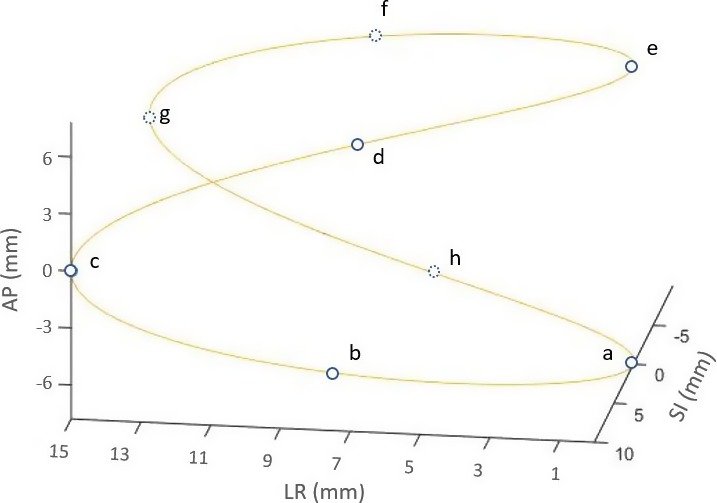
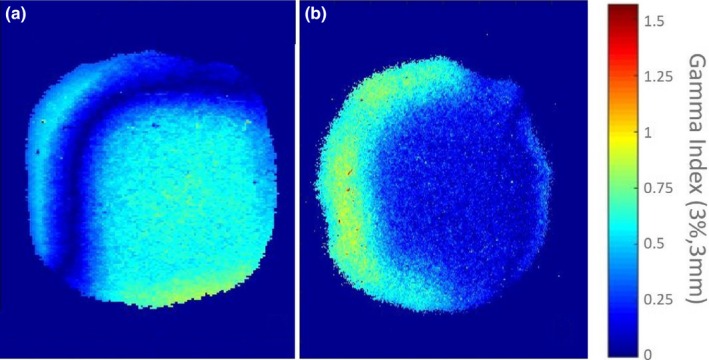
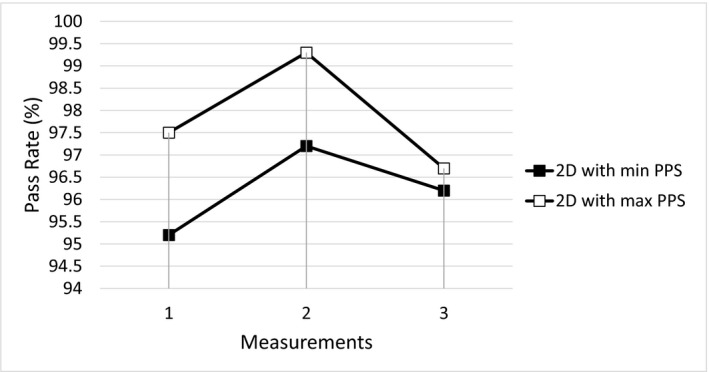
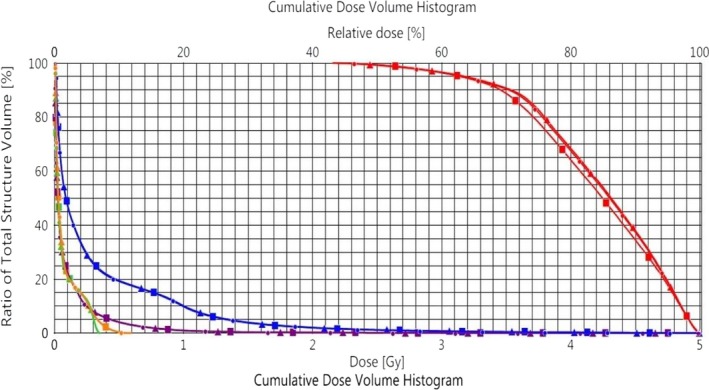
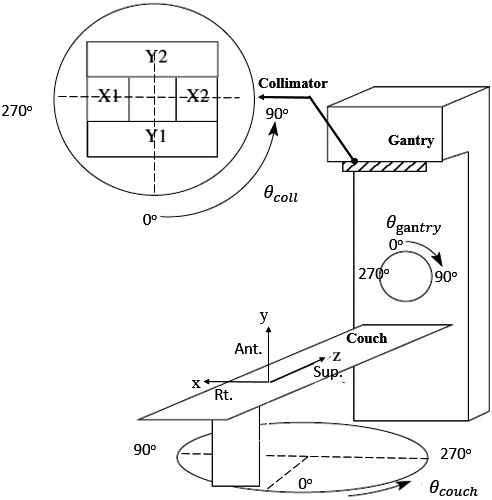
Method and materials: Nontracking conformal arc plans were first created based on a single phase (maximal exhalation phase) of a respiratory motion phantom with a spherical target. An ideal model was used to simulate the target motion in superior-inferior (SI), anterior-posterior (AP), and left-right (LR) dimensions. The motion was decomposed to the MLC leaf position coordinates for motion compensation and generating 4D DCAT plans. The plans were studied with collimator angle ranged from 0° to 90°; couch angle ranged from 350°(-10°) to 10°; and starting tracking phases at maximal inhalation (θ=π/2) and exhalation (θ=0) phases. Plan performance score (PPS) evaluates the plan complexity including the variability in MLC leaf positions, degree of irregularity in field shape and area. PPS ranges from 0 to 1, where low PPS indicates a plan with high complexity. The 4D DCAT plans with the maximal and the minimal PPS were selected and delivered on a Varian TrueBeam linear accelerator. Gafchromic-EBT3 dosimetry films were used to measure the dose delivered to the target in the phantom. Gamma analysis for film measurements with 90% passing rate threshold using 3%/3 mm criteria and trajectory log files were analyzed for plan delivery accuracy evaluation.
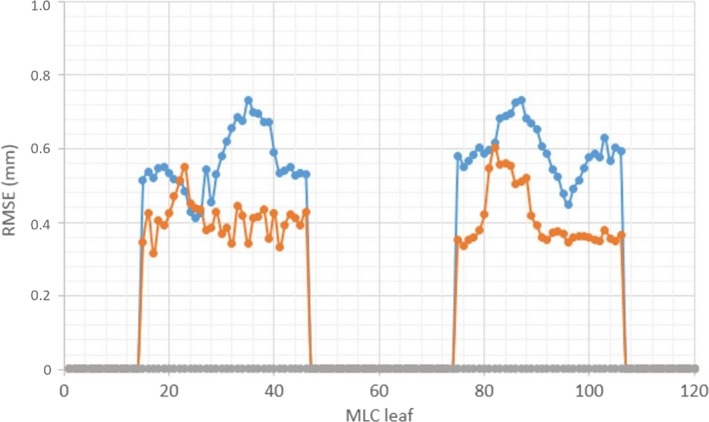
Results: The maximal PPS of all the plans was 0.554, achieved with collimator angle at 87°, couch angle at 350°, and starting phase at maximal inhalation (θ=π/2). The maximal MLC leaf speed, MLC leaf errors, total leaf travel distance, and beam-on time were 20 mm/s, 0.39 ± 0.16 mm, 1385 cm, and 157 s, respectively. The starting phase, whether at maximal inhalation or exhalation had a relatively small contribution to PPS (0.01 ± 0.05).
Conclusions: By selecting collimator angle, couch angle, and starting tracking phase, 4D DCAT plans with the maximal PPS demonstrated less MLC leaf position errors, lower maximal MLC leaf speed, and shorter beam-on time which improved the performance of 4D motion-tracking DCAT delivery.
Keywords: DCAT; MLC; motion tracking.
© 2017 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Figures




References
-
- Nagata Y, Negoro Y, Aoki T, et al. Clinical outcomes of 3D conformal hypofractionated single high‐dose radiotherapy for one or two lung tumors using a stereotactic body frame. Int J Radiat Oncol Biol Phys. 2002;52:1041–1046. - PubMed
-
- Bral S, Parijs HV, Soete G, et al. A feasibility study of image‐guided hypofractionated conformal arc therapy for inoperable patients with localized non‐small cell lung cancer. Radiother Oncol. 2007;84:252–256. - PubMed
-
- Matsuo Y, Takayama K, Nagata Y, et al. Interinstitutional variations in planning for stereotactic body radiation therapy for lung cancer. Int J Radiat Oncol Biol Phys. 2007;68:416–425. - PubMed
-
- Piermattei A, Stimato G, Gaudino D, et al. Dynamic conformal arc therapy: Transmitted signal in vivo dosimetry. Med Phys. 2008;35:1830–1839. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
