

An adapted Clavien-Dindo scoring system in trauma as a clinically meaningful nonmortality endpoint
- PMID: 28731937
- PMCID: PMC5527750
- DOI: 10.1097/TA.0000000000001517
An adapted Clavien-Dindo scoring system in trauma as a clinically meaningful nonmortality endpoint
Abstract
Background: There is no consensus on reporting nonmortality trauma complications in a graded manner. The Clavien-Dindo scale of complications was originally for elective surgery and requires adaptation to provide meaningful data for trauma patients. In particular, the original score does not account for those treated without surgery. We report an adapted Clavien-Dindo in trauma (ACDiT) scale and apply it to patients managed operatively and nonoperatively.
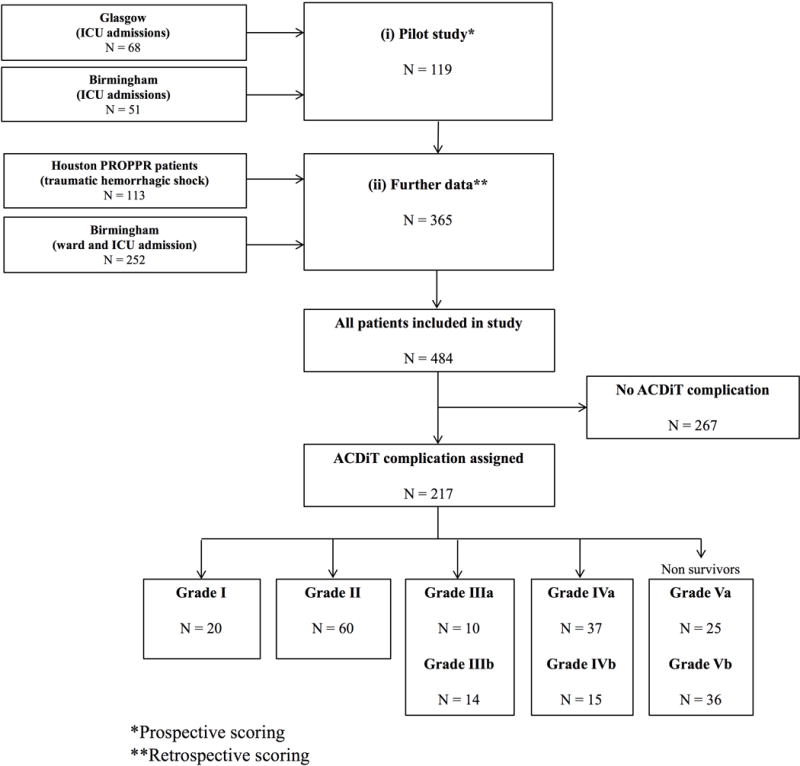
Methods: A combined prospective and retrospective international multicenter observational study was undertaken to apply the ACDiT scale to 484 trauma patients at three university teaching hospitals (Birmingham, England (n = 303); Houston, Texas (n = 113); and Glasgow, Scotland (n = 68)). These included both intensive care unit (ICU) and non-ICU-managed patients. The Clavien-Dindo scoring system was adapted for trauma patients based on consensus amongst an international collaboration of trauma specialists at these sites. Data included whether initial patients were managed operatively or nonoperatively. Complication grades were compared with hospital-free and ICU-free days as other outcome measures of patient morbidity.
Results: Two hundred seventeen (44.8%) of 484 patients experienced complications, of whom 61 (28.1%) of 217 died (grade V). The remainder consisted of grades I (n = 20), II (n = 60), III (n = 24), and IV (n = 52). There was a strong association between higher ACDiT grade category and lower number of hospital-free and ICU-free days (p < 0.01). Eighty-eight patients with complications did not require surgery, validating the score's usefulness in patients managed nonoperatively.
Conclusion: The ACDiT scale can be used to grade the severity of posttrauma complications in patients managed both operatively and nonoperatively. It provides clinically meaningful data for morbidity and mortality meetings and other quality improvement exercises.
Level of evidence: Prognostic, level IV.
Trial registration: ClinicalTrials.gov NCT01545232.
Conflict of interest statement
All authors declare that they have no conflict of interest. Although some authors are affiliated to the UK Defence Medical Services, their opinions are their own, and do not necessarily represent those of the UK Defence Medical Services.
Figures



Similar articles
-
Validation of the Adapted Clavien-Dindo in Trauma (ACDiT) Classifications in Medical and Surgical Management of Acute Diverticulitis.Ann Surg. 2022 Feb 1;275(2):e415-e419. doi: 10.1097/SLA.0000000000003888. Ann Surg. 2022. PMID: 32568744
-
Validation of the adapted clavien dindo in trauma (ACDiT) scale to grade management related complications at a level I trauma center.Turk J Surg. 2022 Dec 20;38(4):391-400. doi: 10.47717/turkjsurg.2022.5793. eCollection 2022 Dec. Turk J Surg. 2022. PMID: 36875271 Free PMC article.
-
Trauma intensive care unit survival: how good is an educated guess?J Trauma. 2010 Jun;68(6):1279-87; discussion 1287-8. doi: 10.1097/TA.0b013e3181de3b99. J Trauma. 2010. PMID: 20539170
-
Morbidity and mortality after distal pancreatectomy for trauma: a critical appraisal of 107 consecutive patients undergoing resection at a Level 1 Trauma Centre.Injury. 2014 Sep;45(9):1401-8. doi: 10.1016/j.injury.2014.04.024. Epub 2014 Apr 16. Injury. 2014. PMID: 24865924 Review.
-
Hypercoagulability and other risk factors in trauma intensive care unit patients with venous thromboembolism.J Trauma Acute Care Surg. 2014 Feb;76(2):443-9. doi: 10.1097/TA.0b013e3182a9d11d. J Trauma Acute Care Surg. 2014. PMID: 24398771
Cited by
-
Survival and neurologic outcomes following aortic occlusion for trauma and hemorrhagic shock in a hybrid operating room.Res Sq [Preprint]. 2023 Jan 13:rs.3.rs-2459030. doi: 10.21203/rs.3.rs-2459030/v1. Res Sq. 2023. Update in: World J Emerg Surg. 2023 Mar 23;18(1):21. doi: 10.1186/s13017-023-00484-w. PMID: 36711502 Free PMC article. Updated. Preprint.
-
In-Hospital Clinical Outcomes in Patients with Fragility Fractures of the Lumbar Spine, Thoracic Spine, and Pelvic Ring: A Comparison of Data before and after Certification as a DGU® Geriatric Trauma Centre.Medicina (Kaunas). 2021 Nov 3;57(11):1197. doi: 10.3390/medicina57111197. Medicina (Kaunas). 2021. PMID: 34833415 Free PMC article.
-
Care of Geriatric Patients with Lumbar Spine, Pelvic, and Acetabular Fractures before and after Certification as a Geriatric Trauma Center DGU®: A Retrospective Cohort Study.Medicina (Kaunas). 2021 Jul 31;57(8):794. doi: 10.3390/medicina57080794. Medicina (Kaunas). 2021. PMID: 34441000 Free PMC article.
-
Severity grading of unexpected events in paediatric surgery: evaluation of five classification systems and the Comprehensive Complication Index (CCI®).BJS Open. 2021 Nov 9;5(6):zrab138. doi: 10.1093/bjsopen/zrab138. BJS Open. 2021. PMID: 35022674 Free PMC article.
-
Hybrid emergency rooms reduce the requirement of blood transfusion in patients with severe trauma.World J Emerg Surg. 2021 Jun 26;16(1):34. doi: 10.1186/s13017-021-00377-w. World J Emerg Surg. 2021. PMID: 34174929 Free PMC article.
References
-
- Holcomb JB, Tilley BC, Baraniuk S, Fox EE, Wade CE, Podbielski JM, del Junco DJ, Brasel KJ, Bulger EM, Callcut RA, et al. Transfusion of plasma, platelets, and red blood cells in a 1:1:1 vs a 1:1:2 ratio and mortality in patients with severe trauma: the PROPPR randomized clinical trial. JAMA. 2015;313(5):471–82. - PMC - PubMed
-
- American College of Surgeons. Committee on Trauma. Resources for optimal care of the injured patient. Chicago, Ill.: American College of Surgeons, Committee on Trauma; 1990.
-
- Sarkar B, Brunsvold ME, Cherry-Bukoweic JR, Hemmila MR, Park PK, Raghavendran K, Wahl WL, Wang SC, Napolitano LM. American College of Surgeons’ Committee on Trauma Performance Improvement and Patient Safety program: maximal impact in a mature trauma center. J Trauma. 2011;71(5):1447–53. discussion 53–4. - PubMed
-
- Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery. 1992;111(5):518–26. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
