

Accuracy and determinants of perceived HIV risk among young women in South Africa
- PMID: 28732496
- PMCID: PMC5520344
- DOI: 10.1186/s12889-017-4593-0
Accuracy and determinants of perceived HIV risk among young women in South Africa
Erratum in
-
Erratum to: BMC Public Health, Vol. 18.BMC Public Health. 2017 Sep 22;17(1):736. doi: 10.1186/s12889-017-4709-6. BMC Public Health. 2017. PMID: 28938882 Free PMC article. No abstract available.
Abstract
Background: HIV risk perceptions are a key determinant of HIV testing. The success of efforts to achieve an AIDS-free generation - including reaching the UNAIDS 90-90-90 target - thus depends critically on the content of these perceptions. We examined the accuracy of HIV-risk perceptions and their correlates among young black women in South Africa, a group with one of the highest HIV incidence rates worldwide.
Methods: We used individual-level longitudinal data from the Cape Area Panel Study (CAPS) from 2005 to 2009 on black African women (20-30 years old in 2009) to assess the association between perceived HIV-risk in 2005 and the probability of testing HIV-positive four years later. We then estimated multivariable logistic regressions using cross-sectional data from the 2009 CAPS wave to assess the relationship between risk perceptions and a wide range of demographic, sexual behaviour and psychosocial covariates of perceived HIV-risk.
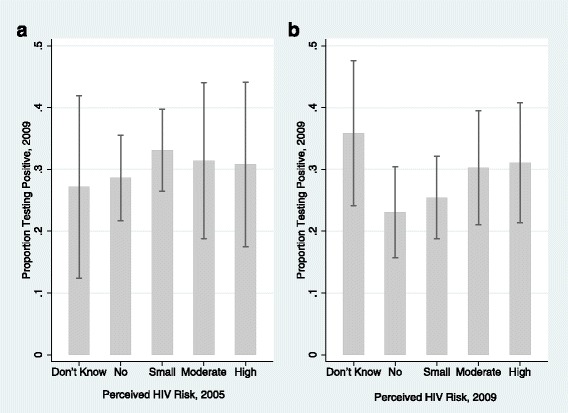
Results: We found that the proportion testing HIV-positive in 2009 was almost identical across perceived risk categories in 2005 (no, small, moderate, great) (χ 2 = 1.43, p = 0.85). Consistent with epidemiologic risk factors, the likelihood of reporting moderate or great HIV-risk perceptions was associated with condom-use (aOR: 0.57; 95% CI: 0.36, 0.89; p < 0.01); having ≥3 lifetime partners (aOR: 2.38, 95% CI: 1.53, 3.73; p < 0.01); knowledge of one's partner's HIV status (aOR: 0.67; 95% CI: 0.43, 1.07; p = 0.09); and being in an age-disparate partnerships (aOR: 1.73; 95% CI: 1.09, 2.76; p = 0.02). However, the likelihood of reporting moderate or great self-perceived risk did not vary with sexually transmitted disease history and respondent age, both strong predictors of HIV risk in the study setting. Risk perceptions were associated with stigmatising attitudes (aOR: 0.53; 95% CI: 0.26, 1.09; p = 0.09); prior HIV testing (aOR: 0.21; 95% CI: 0.13, 0.35; p < 0.01); and having heard that male circumcision is protective (aOR: 0.38; 95% CI: 0.22, 0.64; p < 0.01).
Conclusions: Results indicate that HIV-risk perceptions are inaccurate. Our findings suggest that this inaccuracy stems from HIV-risk perceptions being driven by an incomplete understanding of epidemiological risk and being influenced by a range of psycho-social factors not directly related to sexual behaviour. Consequently, new interventions are needed to align perceived and actual HIV risk.
Keywords: HIV testing; Risk perceptions; Sexual behaviour; South Africa; Stigma; Women.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval for the Cape Area Panel Study was granted by the University of Cape Town and University of Michigan. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Written consent for the surveys was obtained from all respondents, and written parental consent was obtained for interviews with respondents under the age of 18.
Consent for publication
We used de-identified secondary data in our analysis and consequently do not report any individual identifiers in our manuscript.
Competing interests
Both BMB and ASV have no competing interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- UNAIDS: 90–90-90: An ambitious treatment target to help end the AIDS epidemic. In. Edited by Joint United Nations Programme on HIV/AIDS (UNAIDS); 2014: http://www.unaids.org/sites/default/files/media_asset/90-90-90_en_0.pdf.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
