

The Fallacy of Average: How Using HbA1c Alone to Assess Glycemic Control Can Be Misleading
- PMID: 28733374
- PMCID: PMC5521971
- DOI: 10.2337/dc17-0636
The Fallacy of Average: How Using HbA1c Alone to Assess Glycemic Control Can Be Misleading
Abstract
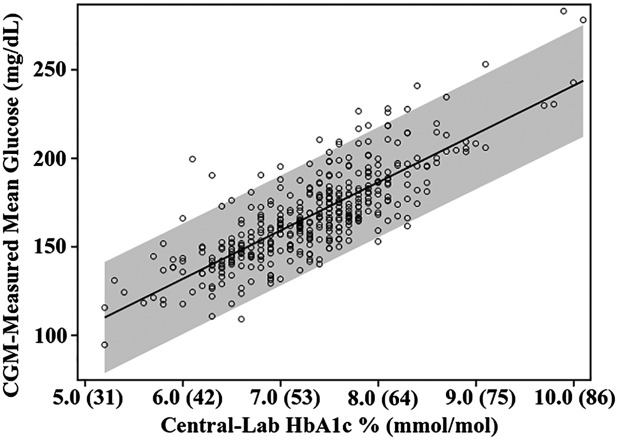
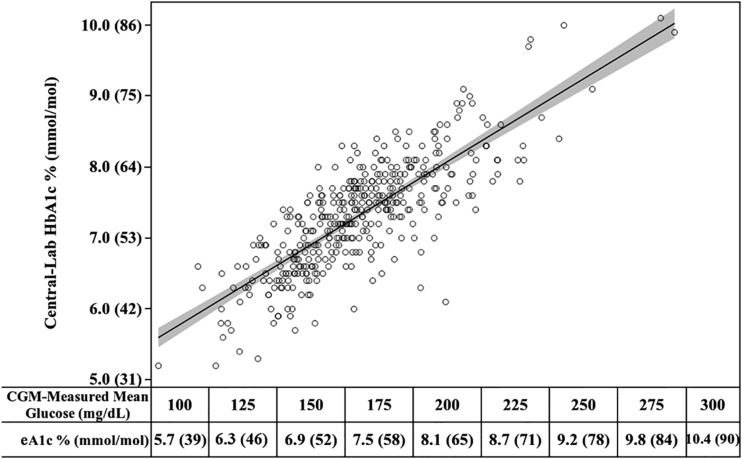
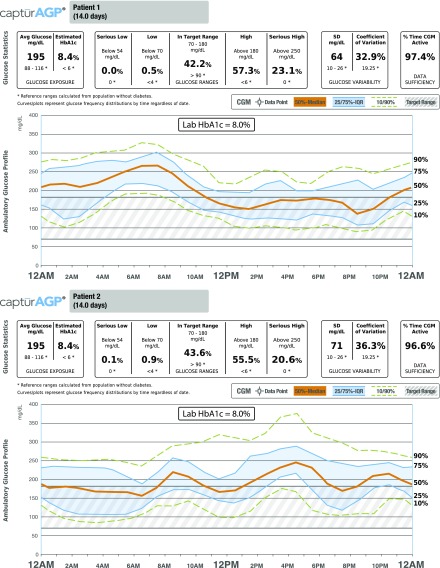
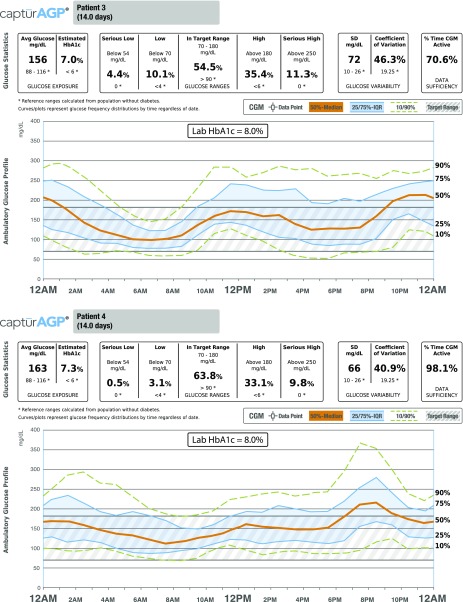
HbA1c is a valuable metric for comparing treatment groups in a randomized trial, for assessing glycemic trends in a population over time, or for cross-sectional comparisons of glycemic control in different populations. However, what is not widely appreciated is that HbA1c may not be a good indicator of an individual patient's glycemic control because of the wide range of mean glucose concentrations and glucose profiles that can be associated with a given HbA1c level. To illustrate this point, we plotted mean glucose measured with continuous glucose monitoring (CGM) versus central laboratory-measured HbA1c in 387 participants in three randomized trials, showing that not infrequently HbA1c may underestimate or overestimate mean glucose, sometimes substantially. Thus, if HbA1c is to be used to assess glycemic control, it is imperative to know the patient's actual mean glucose to understand how well HbA1c is an indicator of the patient's glycemic control. With knowledge of the mean glucose, an estimated HbA1c (eA1C) can be calculated with the formula provided in this article to compare with the measured HbA1c. Estimating glycemic control from HbA1c alone is in essence applying a population average to an individual, which can be misleading. Thus, a patient's CGM glucose profile has considerable value for optimizing his or her diabetes management. In this era of personalized, precision medicine, there are few better examples with respect to the fallacy of applying a population average to a specific patient rather than using specific information about the patient to determine the optimal approach to treatment.
© 2017 by the American Diabetes Association.
Figures
References
-
- Rose T. The End of Average: How We Succeed in a World That Values Sameness. New York, Harper Collins, 2015
-
- Yudkin JS, Forrest RD, Jackson CA, Ryle AJ, Davie S, Gould BJ. Unexplained variability of glycated haemoglobin in non-diabetic subjects not related to glycaemia. Diabetologia 1990;33:208–215 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
