

Atherogenic Lipoprotein Determinants of Cardiovascular Disease and Residual Risk Among Individuals With Low Low-Density Lipoprotein Cholesterol
- PMID: 28733430
- PMCID: PMC5586287
- DOI: 10.1161/JAHA.117.005549
Atherogenic Lipoprotein Determinants of Cardiovascular Disease and Residual Risk Among Individuals With Low Low-Density Lipoprotein Cholesterol
Abstract
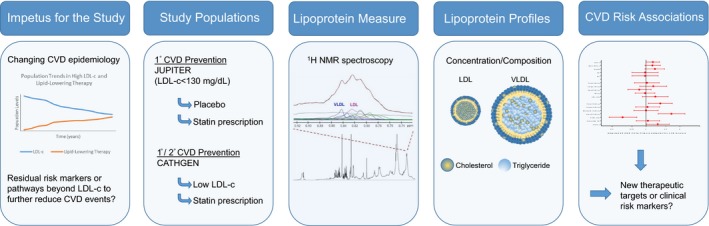
Background: Levels of LDL (low-density lipoprotein) cholesterol in the population are declining, and increasing attention is being focused on residual lipid-related pathways of atherosclerotic cardiovascular disease risk beyond LDL cholesterol. Among individuals with low (<130 mg/dL) LDL cholesterol, we undertook detailed profiling of circulating atherogenic lipoproteins in relation to incident cardiovascular disease in 2 populations.
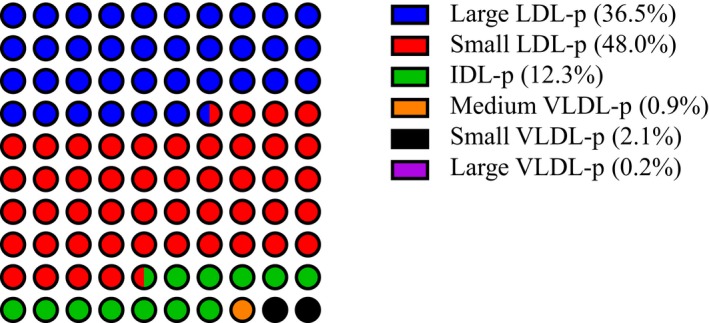
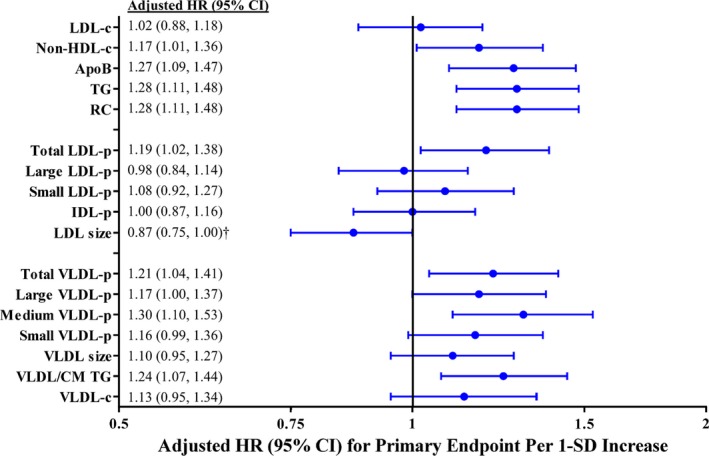
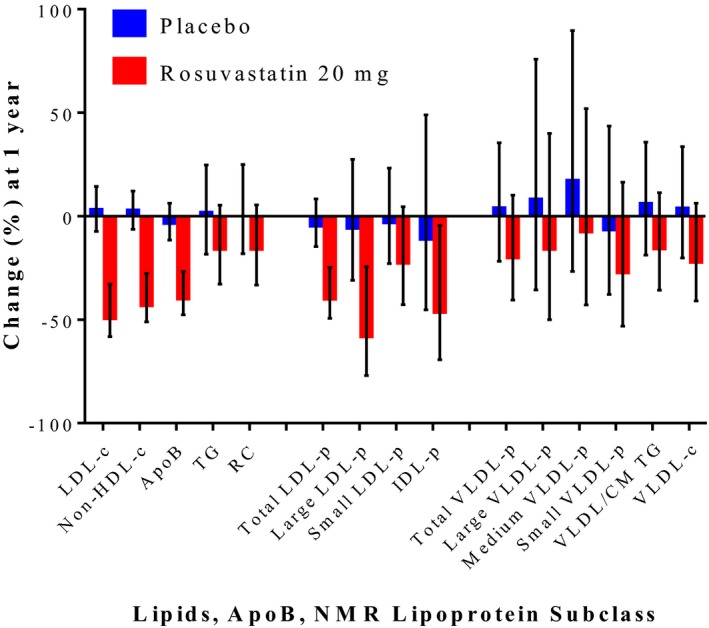
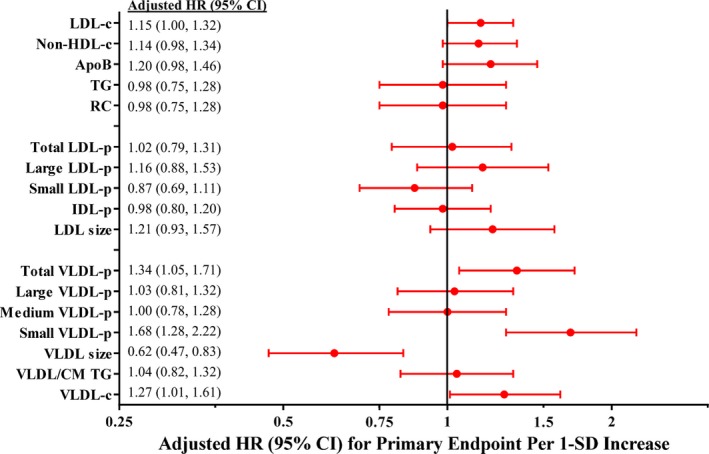
Methods and results: We performed proton nuclear magnetic resonance spectroscopy to quantify concentrations of LDL and VLDL (very low-density lipoprotein) particle subclasses in 11 984 JUPITER trial participants (NCT00239681). Adjusted Cox models examined cardiovascular disease risk associated with lipoprotein measures according to treatment allocation. Risk (adjusted hazard ratio [95%CI] per SD increment) among placebo-allocated participants was associated with total LDL particles (1.19 [1.02, 1.38]) and total VLDL particles (1.21 [1.04, 1.41]), as well as apolipoprotein B, non-high-density lipoprotein cholesterol, and triglycerides, but not LDL-c. Rosuvastatin reduced LDL measures but had variable effects on triglyceride and VLDL measures. On-statin levels of the smallest VLDL particle subclass were associated with a 68% per-SD (adjusted hazard ratio 1.68 [1.28, 2.22]) increase in residual risk-this risk was related to VLDL cholesterol and not triglyceride or larger VLDL particles. There was evidence that residual risk prediction during statin therapy could be significantly improved through the inclusion of key VLDL measures (Harrell C-index 0.780 versus 0.712; P<0.0001). In an independent, prospective cohort of 4721 individuals referred for cardiac catheterization (CATHGEN), similar patterns of lipoprotein-related risk were observed.
Conclusions: Atherogenic lipoprotein particle concentrations were associated with cardiovascular disease risk when LDL cholesterol was low. VLDL lipoproteins, particularly the smallest remnant subclass, may represent unused targets for risk prediction and potential therapeutic intervention for reducing residual risk.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00239681.
Keywords: atherosclerosis; lipids and lipoproteins; metabolomics; nuclear magnetic resonance spectroscopy; prevention.
© 2017 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Kuklina EV, Yoon PW, Keenan NL. Trends in high levels of low‐density lipoprotein cholesterol in the United States, 1999–2006. JAMA. 2009;302:2104–2110. - PubMed
-
- Baigent C, Keech A, Kearney PM, Blackwell L, Buck G, Pollicino C, Kirby A, Sourjina T, Peto R, Collins R, Simes R; Cholesterol Treatment Trialists' Collaborators . Efficacy and safety of cholesterol‐lowering treatment: prospective meta‐analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- van Lammeren GW, den Ruijter HM, Vrijenhoek JE, van der Laan SW, Velema E, de Vries JP, de Kleijn DP, Vink A, de Borst GJ, Moll FL, Bots ML, Pasterkamp G. Time‐dependent changes in atherosclerotic plaque composition in patients undergoing carotid surgery. Circulation. 2014;129:2269–2276. - PubMed
-
- Libby P, Pasterkamp G. Requiem for the ‘vulnerable plaque’. Eur Heart J. 2015;36:2984–2987. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
