

Safety Profile and Immunologic Responses of a Novel Vaccine Against Shigella sonnei Administered Intramuscularly, Intradermally and Intranasally: Results From Two Parallel Randomized Phase 1 Clinical Studies in Healthy Adult Volunteers in Europe
- PMID: 28735965
- PMCID: PMC5552227
- DOI: 10.1016/j.ebiom.2017.07.013
Safety Profile and Immunologic Responses of a Novel Vaccine Against Shigella sonnei Administered Intramuscularly, Intradermally and Intranasally: Results From Two Parallel Randomized Phase 1 Clinical Studies in Healthy Adult Volunteers in Europe
Abstract
Background: Approximately 164,000 deaths yearly are due to shigellosis, primarily in developing countries. Thus, a safe and affordable Shigella vaccine is an important public health priority. The GSK Vaccines Institute for Global Health (GVGH) developed a candidate Shigella sonnei vaccine (1790GAHB) using the Generalized Modules for Membrane Antigens (GMMA) technology. The paper reports results of 1790GAHB Phase 1 studies in healthy European adults.
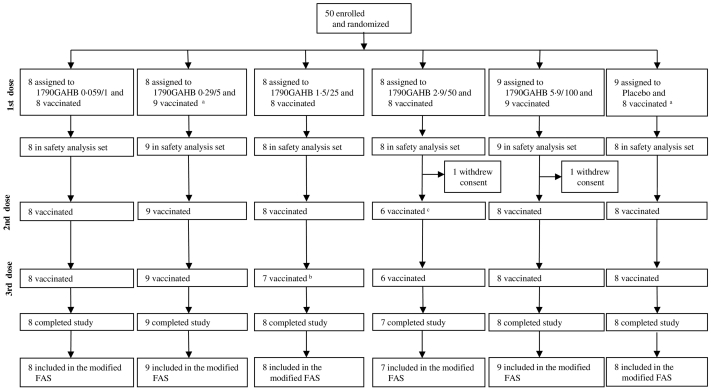
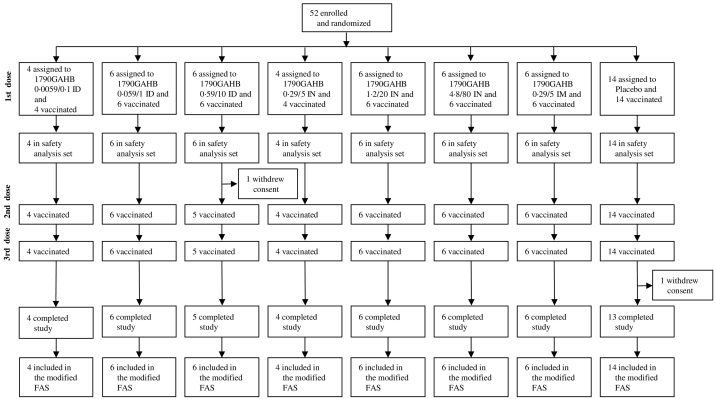
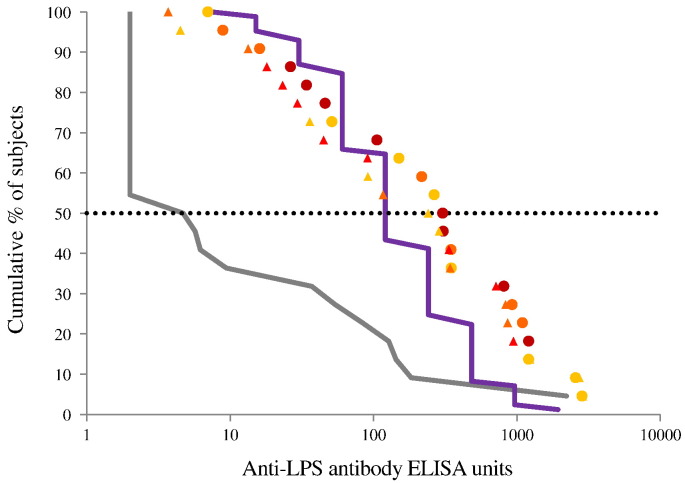
Methods: To evaluate the safety and immunogenicity profiles of 1790GAHB, we performed two parallel, phase 1, observer-blind, randomized, placebo-controlled, dose escalation studies in France ("study 1") and the United Kingdom ("study 2") between February 2014 and April 2015 (ClinicalTrials.gov, number NCT02017899 and NCT02034500, respectively) in 18-45years old subjects (50 in study 1, 52 in study 2). Increasing doses of Alhydrogel adsorbed 1790, expressed by both O Antigen (OAg) and protein quantity, or placebo were given either by intramuscular route (0.059/1, 0.29/5, 1.5/25, 2.9/50, 5.9/100μg of OAg/μg of protein; study 1) or by intradermal (ID), intranasal (IN) or intramuscular (IM) route of immunization (0.0059/0.1, 0.059/1, 0.59/10μg ID, 0.29/5, 1.2/20, 4.8/80μg IN and 0.29/5μg IM, respectively; study 2). In absence of serologic correlates of protection for Shigella sonnei, vaccine induced immunogenicity was compared to anti-LPS antibody in a population naturally exposed to S. sonnei.
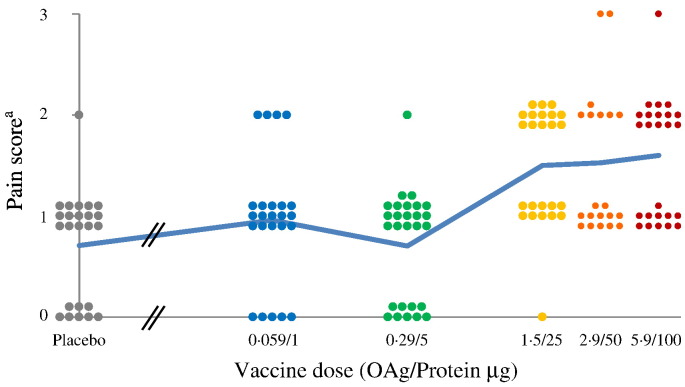
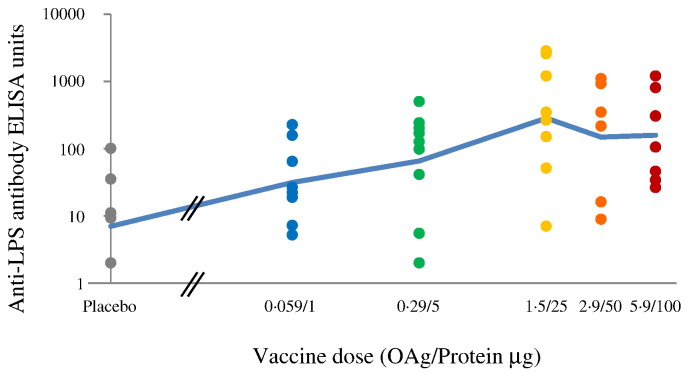
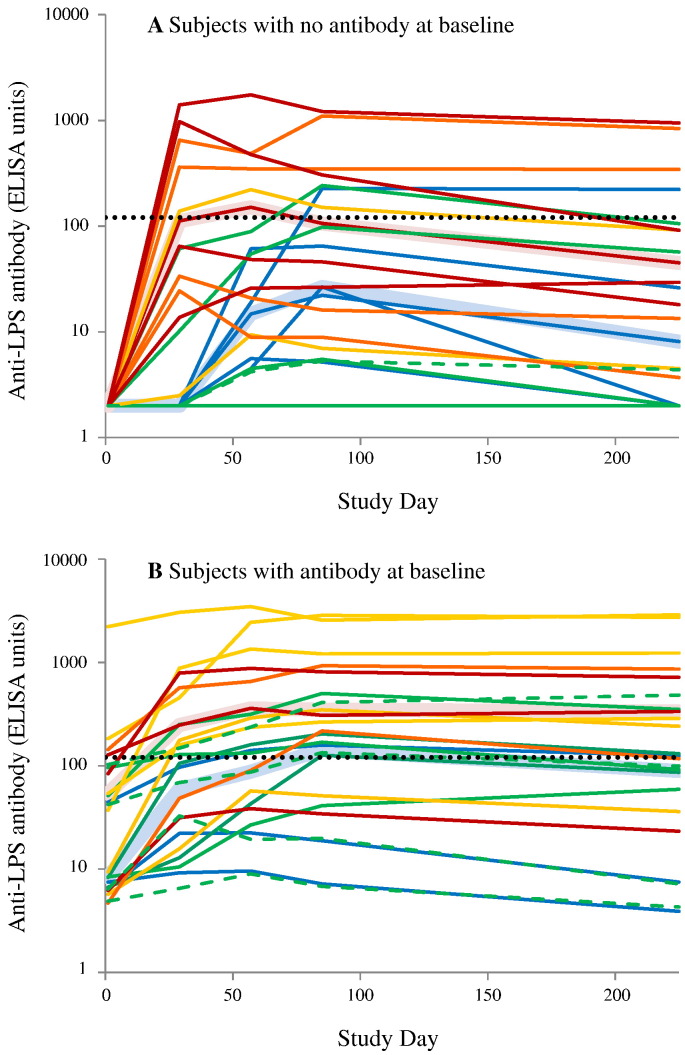
Findings: Vaccines were well tolerated in both studies and no death or vaccine related serious adverse events were reported. In study 1, doses ≥1.5/25μg elicited serum IgG median antibody greater than median level in convalescent subjects after the first dose. No vaccine group in study 2 achieved median antibody greater than the median convalescent antibody.
Interpretation: Intramuscularly administered Shigella sonnei GMMA vaccine is well tolerated, up to and including 5.9/100μg and induces antibody to the OAg of at least the same magnitude of those observed following natural exposure to the pathogen. Vaccine administered by ID or IN, although well tolerated, is poorly immunogenic at the doses delivered. The data support the use of the GMMA technology for the development of intramuscular multivalent Shigella vaccines.
Keywords: Clinical study; GMMA; Shigella sonnei; Vaccine.
Copyright © 2017 GlaxoSmithKline SA. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Camacho A.I., Irache J.M., Gamazo C. Recent progress towards development of a Shigella vaccine. Expert Rev. Vaccines. 2013;12(1):43–55. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
