

Thromboembolic Risk, Bleeding Outcomes and Effect of Different Antithrombotic Strategies in Very Elderly Patients With Atrial Fibrillation: A Sub-Analysis From the PREFER in AF (PRE vention o F Thromboembolic Events- E uropean R egistry in A trial F ibrillation)
- PMID: 28736385
- PMCID: PMC5586290
- DOI: 10.1161/JAHA.117.005657
Thromboembolic Risk, Bleeding Outcomes and Effect of Different Antithrombotic Strategies in Very Elderly Patients With Atrial Fibrillation: A Sub-Analysis From the PREFER in AF (PRE vention o F Thromboembolic Events- E uropean R egistry in A trial F ibrillation)
Abstract
Background: Increasing age predisposes to both thromboembolic and bleeding events in patients with atrial fibrillation; therefore, balancing risks and benefits of antithrombotic strategies in older populations is crucial. We investigated 1-year outcome with different antithrombotic approaches in very elderly atrial fibrillation patients (age ≥85 years) compared with younger patients.
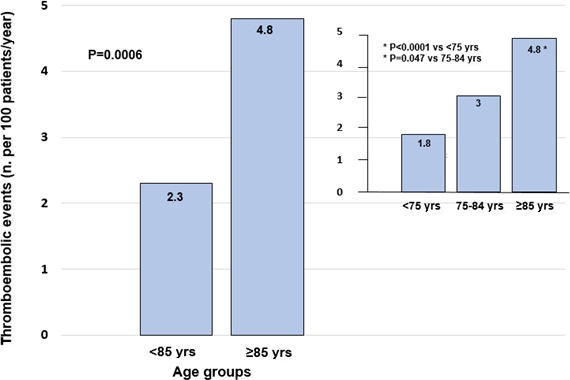
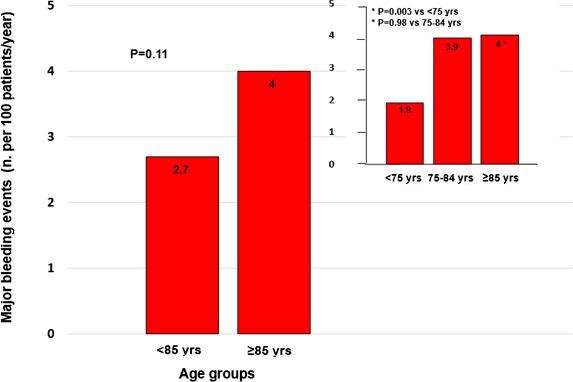
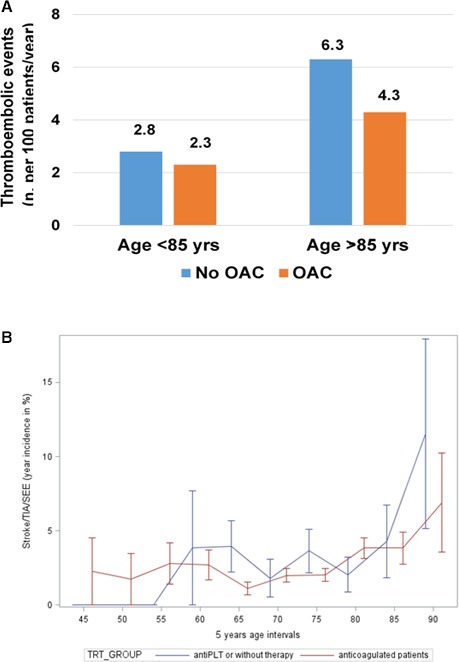
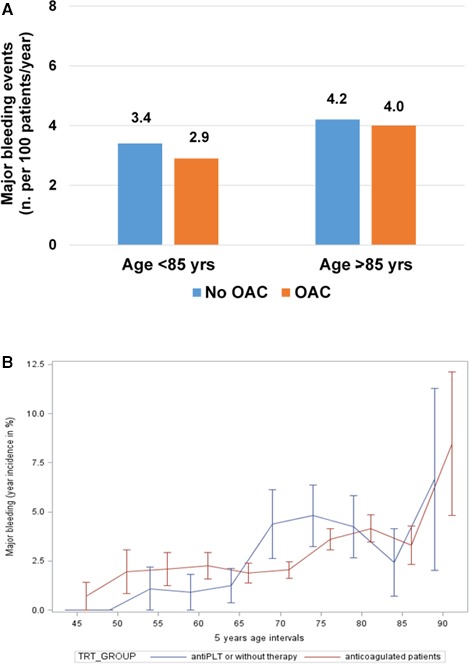
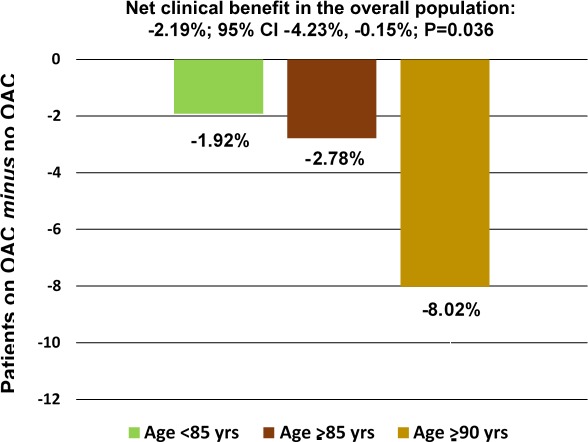
Methods and results: We accessed individual patients' data from the prospective PREFER in AF (PREvention oF thromboembolic events-European Registry in Atrial Fibrillation), compared outcomes with and without oral anticoagulation (OAC), and estimated weighed net clinical benefit in different age groups. A total of 6412 patients, 505 of whom were aged ≥85 years, were analyzed. In patients aged <85 years, the incidence of thromboembolic events was 2.8%/year without OAC versus 2.3%/year with OAC (0.5% absolute reduction); in patients aged ≥85 years, it was 6.3%/year versus 4.3%/year (2% absolute reduction). In very elderly patients, the risk of major bleeding was higher than in younger patients, but similar in patients on OAC and in those on antiplatelet therapy or without antithrombotic treatment (4.0%/year versus 4.2%/year; P=0.77). OAC was overall associated with weighted net clinical benefit, assigning weights to nonfatal events according to their prognostic implication for subsequent death (-2.19%; CI, -4.23%, -0.15%; P=0.036). We found a significant gradient of this benefit as a function of age, with the oldest patients deriving the highest benefit.
Conclusions: Because the risk of stroke increases with age more than the risk of bleeding, the absolute benefit of OAC is highest in very elderly patients, where it, by far, outweighs the risk of bleeding, with the greatest net clinical benefit in such patients.
Keywords: anticoagulation; atrial fibrillation; major bleeding; thromboembolic events; very elderly.
© 2017 The Authors and Daiichi Sankyo Europe GmbH. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
Comment in
-
Stroke Prevention in Atrial Fibrillation in the Very Elderly: Anticoagulant Therapy Is No Longer a Sin.J Am Heart Assoc. 2017 Jul 23;6(7):e006864. doi: 10.1161/JAHA.117.006864. J Am Heart Assoc. 2017. PMID: 28736386 Free PMC article. No abstract available.
References
-
- National Population Projections 2010‐Based Statistical Bulletin. London: Office for National Statistics; 2011. Available at: http://www.ons.gov.uk/ons/dcp171778_235886.pdf. Accessed November 1, 2016.
-
- Andreotti F, Rocca B, Husted S, Ajjan RA, ten Berg J, Cattaneo M, Collet JP, De Caterina R, Fox KAA, Halvorsen S, Huber K, Hylek EM, Lip GYH, Montalescot G, Morais J, Patrono C, Verheugt FWA, Wallentin L, Weiss TW, Storey RF; on behalf of the ESC Thrombosis Working Group . Antithrombotic therapy in the elderly: expert position paper of the European Society of Cardiology Working Group on Thrombosis. Eur Heart J. 2015;36:3238–3249. - PubMed
-
- Marinigh R, Lip GYH, Fiotti N, Giansante C, Lane DA. Age as a risk factor for stroke in atrial fibrillation patients. J Am Coll Cardiol. 2010;56:827–837. - PubMed
-
- Mant J, Hobbs R, Fletcher K, Roalfe A, Fitzmaurice D, Lip GYH, Murray E. Warfarin versus aspirin for stroke prevention in an elderly community population with atrial fibrillation (the Birmingham Atrial Fibrillation Treatment of the Aged study, BAFTA): a randomized controlled trial. Lancet. 2007;370:493–503. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
