

Investigating the Impact of Different Suspicion of Infection Criteria on the Accuracy of Quick Sepsis-Related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores
- PMID: 28737573
- PMCID: PMC5640476
- DOI: 10.1097/CCM.0000000000002648
Investigating the Impact of Different Suspicion of Infection Criteria on the Accuracy of Quick Sepsis-Related Organ Failure Assessment, Systemic Inflammatory Response Syndrome, and Early Warning Scores
Abstract
Objective: Studies in sepsis are limited by heterogeneity regarding what constitutes suspicion of infection. We sought to compare potential suspicion criteria using antibiotic and culture order combinations in terms of patient characteristics and outcomes. We further sought to determine the impact of differing criteria on the accuracy of sepsis screening tools and early warning scores.
Design: Observational cohort study.
Setting: Academic center from November 2008 to January 2016.
Patients: Hospitalized patients outside the ICU.
Interventions: None.
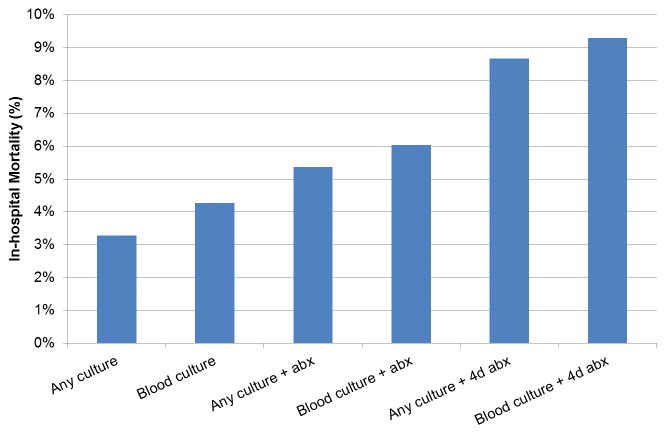
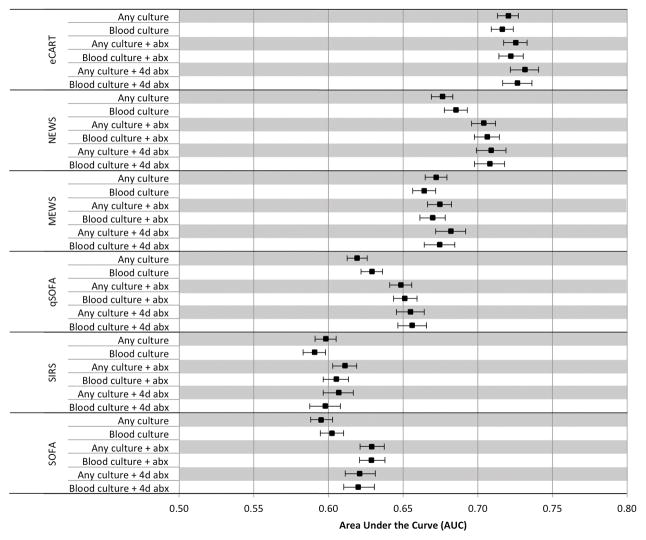
Measurements and main results: Six criteria were investigated: 1) any culture, 2) blood culture, 3) any culture plus IV antibiotics, 4) blood culture plus IV antibiotics, 5) any culture plus IV antibiotics for at least 4 of 7 days, and 6) blood culture plus IV antibiotics for at least 4 of 7 days. Accuracy of the quick Sepsis-related Organ Failure Assessment score, Sepsis-related Organ Failure Assessment score, systemic inflammatory response syndrome criteria, the National and Modified Early Warning Score, and the electronic Cardiac Arrest Risk Triage score were calculated for predicting ICU transfer or death within 48 hours of meeting suspicion criteria. A total of 53,849 patients met at least one infection criteria. Mortality increased from 3% for group 1 to 9% for group 6 and percentage meeting Angus sepsis criteria increased from 20% to 40%. Across all criteria, score discrimination was lowest for systemic inflammatory response syndrome (median area under the receiver operating characteristic curve, 0.60) and Sepsis-related Organ Failure Assessment score (median area under the receiver operating characteristic curve, 0.62), intermediate for quick Sepsis-related Organ Failure Assessment (median area under the receiver operating characteristic curve, 0.65) and Modified Early Warning Score (median area under the receiver operating characteristic curve 0.67), and highest for National Early Warning Score (median area under the receiver operating characteristic curve 0.71) and electronic Cardiac Arrest Risk Triage (median area under the receiver operating characteristic curve 0.73).
Conclusions: The choice of criteria to define a potentially infected population significantly impacts prevalence of mortality but has little impact on accuracy. Systemic inflammatory response syndrome was the least predictive and electronic Cardiac Arrest Risk Triage the most predictive regardless of how infection was defined.
Figures
Comment in
-
Machine Learning and Sepsis: On the Road to Revolution.Crit Care Med. 2017 Nov;45(11):1946-1947. doi: 10.1097/CCM.0000000000002673. Crit Care Med. 2017. PMID: 29028697 Free PMC article. No abstract available.
References
-
- Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312(1):90–92. - PubMed
-
- Lagu T, Rothberg MB, Shieh MS, et al. Hospitalizations, costs, and outcomes of severe sepsis in the United States 2003 to 2007. Crit Care Med. 2012;40(3):754–761. - PubMed
-
- Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41(2):580–637. - PubMed
-
- Angus DC, Linde-Zwirble WT, Lidicker J, et al. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303–1310. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
