

Prostate-Specific Membrane Antigen-Targeted Imaging With [18F]DCFPyL in High-Grade Gliomas
- PMID: 28737579
- PMCID: PMC5802343
- DOI: 10.1097/RLU.0000000000001769
Prostate-Specific Membrane Antigen-Targeted Imaging With [18F]DCFPyL in High-Grade Gliomas
Abstract
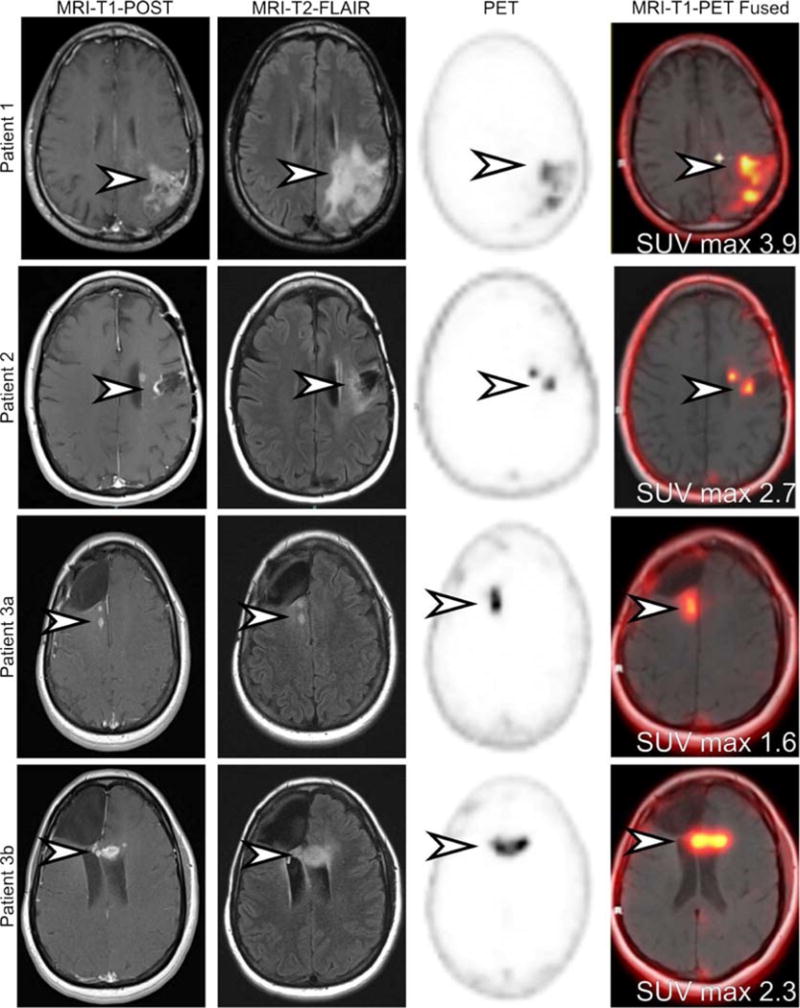
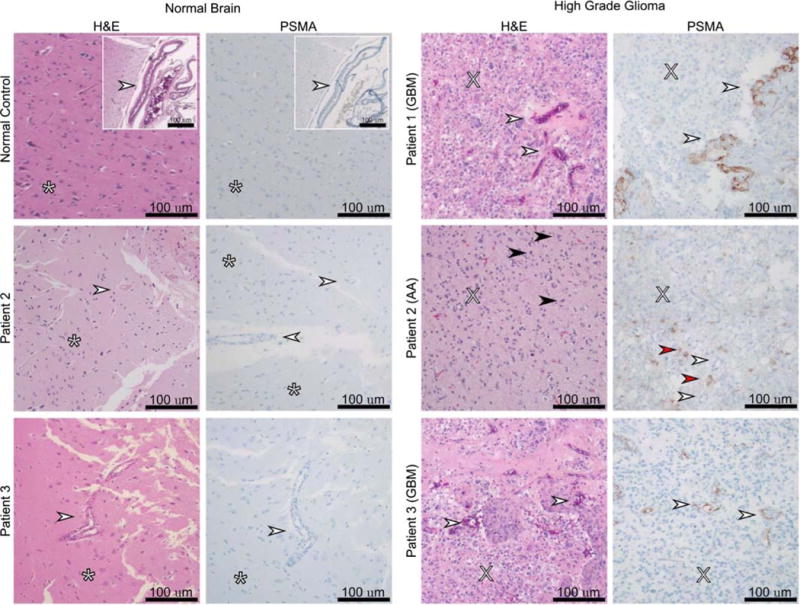
High-grade gliomas (World Health Organization grade III-IV) are highly lethal primary brain tumors. Imaging modalities, including MRI and FDG PET, provide a limited ability to differentiate treatment effects (such as radiation necrosis) from recurrent or residual tumor. As the first step in validating the applicability of prostate-specific membrane antigen (PSMA)-targeted imaging in high-grade gliomas, we evaluated the ability of the PSMA-targeted small molecule [F]DCFPyL (2-(3-(1carboxy-5-(6-[F]fluoro-pyridine-3-carbonyl)-amino]-pentyl)-ureido)-pentanedioic acid) to image high-grade gliomas in a series of 3 prospectively recruited patients. We found [F]DCFPyL binds PSMA in the neovasculature of glioblastoma multiforme and tumor cells of anaplastic astrocytoma.
Conflict of interest statement
Conflicts of interest: This arrangement has been reviewed and approved by the Johns Hopkins University in accordance with its conflict of interest policies. The other authors have none declared.
Figures
References
-
- Schwenck J, Tabatabai G, Skardelly M, et al. In vivo visualization of prostate-specific membrane antigen in glioblastoma. Eur J Nucl Med Mol Imaging. 2015;42:170–171. - PubMed
-
- Sasikumar A, Joy A, Pillai MR, et al. Diagnostic value of 68Ga PSMA-11 PET/CT imaging of brain tumors—preliminary analysis. Clin Nucl Med. 2017;42:e41–e48. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
