

Identifying Risk for Acute Kidney Injury in Infants and Children Following Cardiac Arrest
- PMID: 28737594
- PMCID: PMC5628129
- DOI: 10.1097/PCC.0000000000001280
Identifying Risk for Acute Kidney Injury in Infants and Children Following Cardiac Arrest
Abstract
Objectives: Our goal was to identify risk factors for acute kidney injury in children surviving cardiac arrest.
Design: Retrospective analysis of a public access dataset.
Setting: Fifteen children's hospitals associated with the Pediatric Emergency Care Applied Research Network.
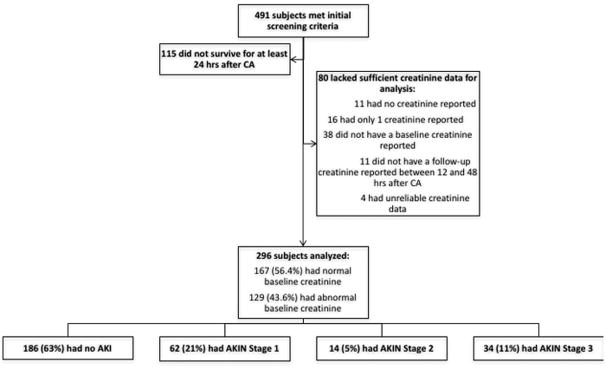
Patients: Two hundred ninety-six subjects between 1 day and 18 years old who experienced in-hospital or out-of-hospital cardiac arrest between July 1, 2003, and December 31, 2004.
Interventions: None.
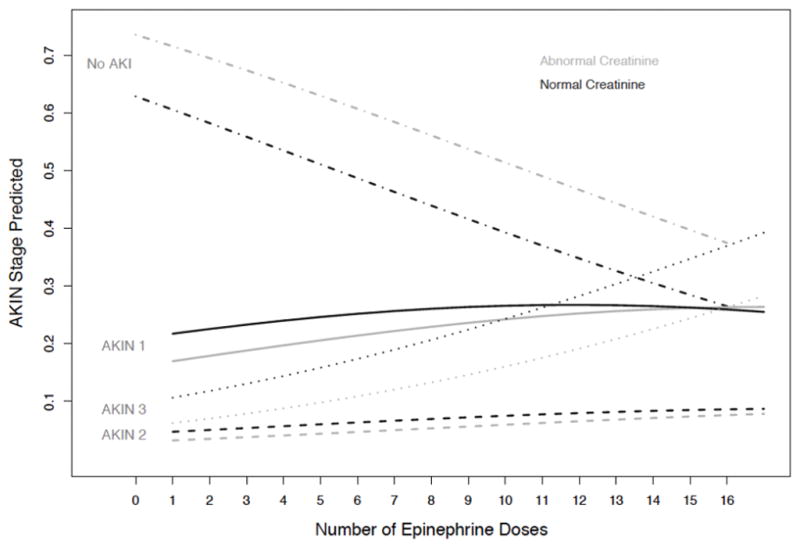
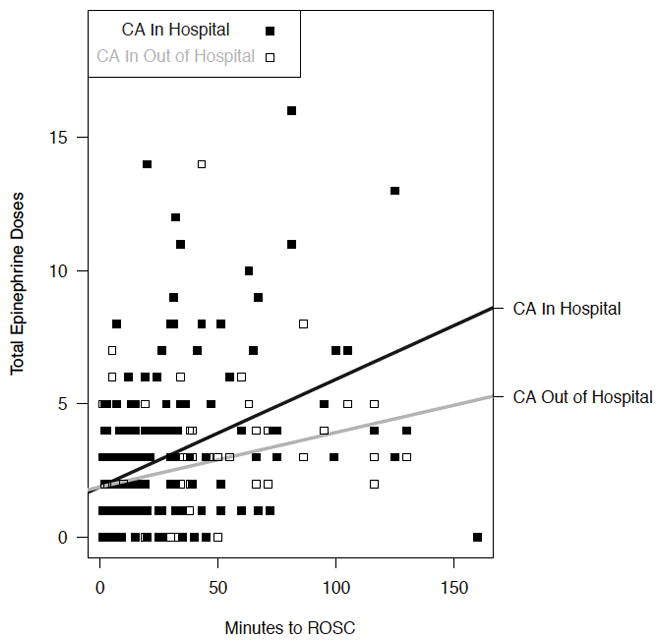
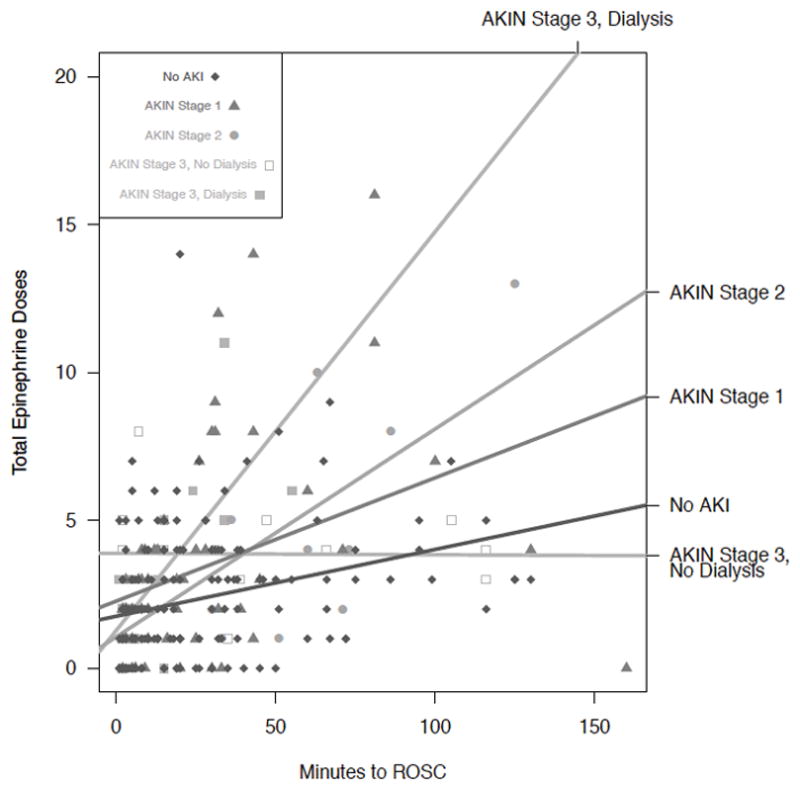
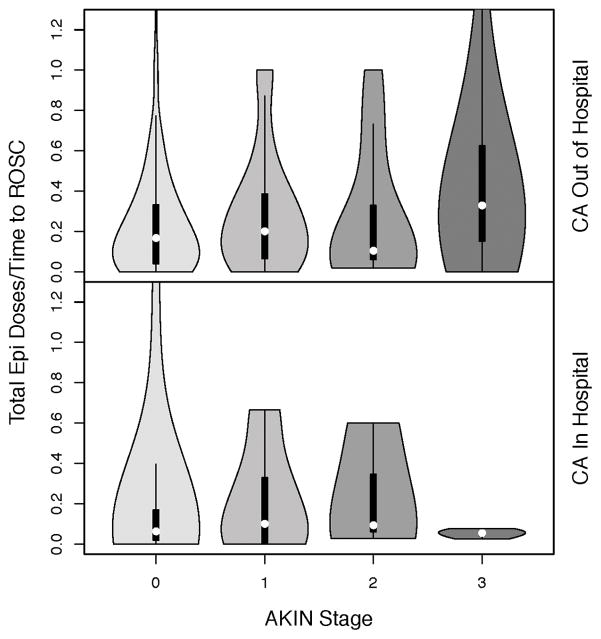
Measurements and main results: Our primary outcome was development of acute kidney injury as defined by the Acute Kidney Injury Network criteria. An ordinal probit model was developed. We found six critical explanatory variables, including total number of epinephrine doses, postcardiac arrest blood pressure, arrest location, presence of a chronic lung condition, pH, and presence of an abnormal baseline creatinine. Total number of epinephrine doses received as well as rate of epinephrine dosing impacted acute kidney injury risk and severity of acute kidney injury.
Conclusions: This study is the first to identify risk factors for acute kidney injury in children after cardiac arrest. Our findings regarding the impact of epinephrine dosing are of particular interest and suggest potential for epinephrine toxicity with regard to acute kidney injury. The ability to identify and potentially modify risk factors for acute kidney injury after cardiac arrest may lead to improved morbidity and mortality in this population.
Figures
Comment in
-
"I Saw the Light" (1): Hank Williams Sr, Acute Kidney Injury, and Cardiopulmonary Arrest.Pediatr Crit Care Med. 2017 Oct;18(10):997-998. doi: 10.1097/PCC.0000000000001289. Pediatr Crit Care Med. 2017. PMID: 28976468 No abstract available.
References
-
- Clermont G, Acker CG, Angus DC, et al. Renal failure in the ICU: comparison of the impact of acute renal failure and end-stage renal disease on ICU outcomes. Kidney International. 2002;62:986–996. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
