

Optimization and Interpretation of Serial QuantiFERON Testing to Measure Acquisition of Mycobacterium tuberculosis Infection
- PMID: 28737960
- PMCID: PMC5620669
- DOI: 10.1164/rccm.201704-0817OC
Optimization and Interpretation of Serial QuantiFERON Testing to Measure Acquisition of Mycobacterium tuberculosis Infection
Abstract
Rationale: Conversion from a negative to positive QuantiFERON-TB test is indicative of Mycobacterium tuberculosis (Mtb) infection, which predisposes individuals to tuberculosis disease. Interpretation of serial tests is confounded by immunological and technical variability.
Objectives: To improve the consistency of serial QuantiFERON-TB testing algorithms and provide a data-driven definition of conversion.
Methods: Sources of QuantiFERON-TB variability were assessed, and optimal procedures were identified. Distributions of IFN-γ response levels were analyzed in healthy adolescents, Mtb-unexposed control subjects, and patients with pulmonary tuberculosis.
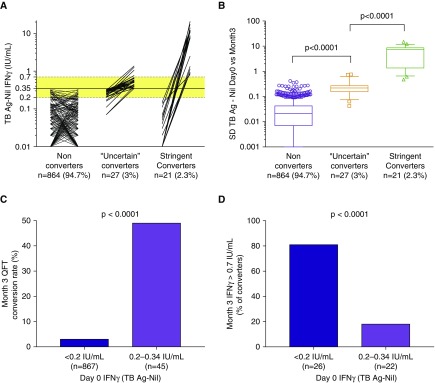
Measurements and main results: Individuals with no known Mtb exposure had IFN-γ values less than 0.2 IU/ml. Among individuals with IFN-γ values less than 0.2 IU/ml, 0.2-0.34 IU/ml, 0.35-0.7 IU/ml, and greater than 0.7 IU/ml, tuberculin skin test positivity results were 15%, 53%, 66%, and 91% (P < 0.005), respectively. Together, these findings suggest that values less than 0.2 IU/ml were true negatives. In short-term serial testing, "uncertain" conversions, with at least one value within the uncertainty zone (0.2-0.7 IU/ml), were partly explained by technical assay variability. Individuals who had a change in QuantiFERON-TB IFN-γ values from less than 0.2 to greater than 0.7 IU/ml had 10-fold higher tuberculosis incidence rates than those who maintained values less than 0.2 IU/ml over 2 years (P = 0.0003). By contrast, "uncertain" converters were not at higher risk than nonconverters (P = 0.229). Eighty-seven percent of patients with active tuberculosis had IFN-γ values greater than 0.7 IU/ml, suggesting that these values are consistent with established Mtb infection.
Conclusions: Implementation of optimized procedures and a more rigorous QuantiFERON-TB conversion definition (an increase from IFN-γ <0.2 to >0.7 IU/ml) would allow more definitive detection of recent Mtb infection and potentially improve identification of those more likely to develop disease.
Keywords: IFN-γ release assay; QuantiFERON; conversion; tuberculosis; variability.
Figures





Comment in
-
Detecting New Mycobacterium tuberculosis Infection. Time for a More Nuanced Interpretation of QuantiFERON Conversions.Am J Respir Crit Care Med. 2017 Sep 1;196(5):546-547. doi: 10.1164/rccm.201707-1543ED. Am J Respir Crit Care Med. 2017. PMID: 28763239 No abstract available.
References
-
- Machingaidze S, Verver S, Mulenga H, Abrahams DA, Hatherill M, Hanekom W, Hussey GD, Mahomed H. Predictive value of recent QuantiFERON conversion for tuberculosis disease in adolescents. Am J Respir Crit Care Med. 2012;186:1051–1056. - PubMed
-
- World Health Organization (WHO) Guidelines on the management of latent tuberculosis infection. Geneva, Switzerland: WHO; 2015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
