

Impact of a Patient Support Program on Patient Adherence to Adalimumab and Direct Medical Costs in Crohn's Disease, Ulcerative Colitis, Rheumatoid Arthritis, Psoriasis, Psoriatic Arthritis, and Ankylosing Spondylitis
- PMID: 28737994
- PMCID: PMC10397981
- DOI: 10.18553/jmcp.2017.16272
Impact of a Patient Support Program on Patient Adherence to Adalimumab and Direct Medical Costs in Crohn's Disease, Ulcerative Colitis, Rheumatoid Arthritis, Psoriasis, Psoriatic Arthritis, and Ankylosing Spondylitis
Abstract
Background: AbbVie provides a free-to-patient patient support program (PSP) to assist adalimumab-treated patients with medication costs, nurse support, injection training, pen disposal, and medication reminders. The impact of these services on patient adherence to adalimumab and direct medical costs associated with autoimmune disease has not been assessed.
Objective: To quantify the relationship between participation in a PSP and outcomes (adalimumab adherence, persistence, and direct medical costs) in patients initiating adalimumab treatment.
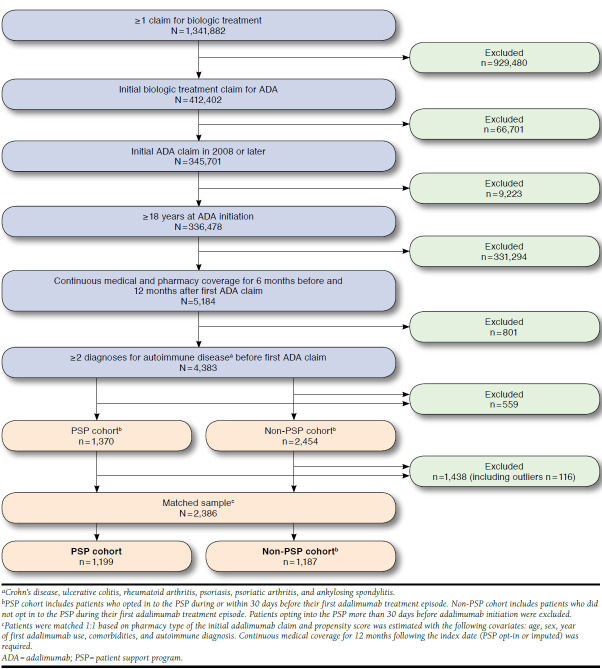
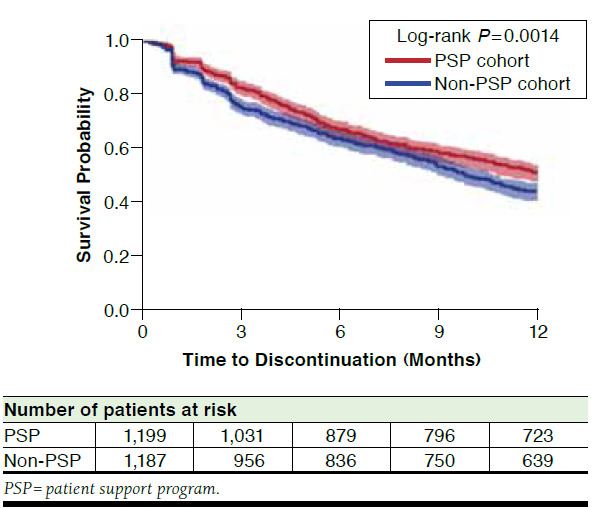
Methods: A longitudinal, retrospective, cohort study was conducted using patient-level data from the PSP combined with Symphony Health Solutions administrative claims data for patients initiating adalimumab between January 2008 and June 2014. The sample included patients aged ≥ 18 years with a diagnosis of Crohn's disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, or ankylosing spondylitis who were biologic-naïve before initiation of adalimumab. Patients who enrolled in the PSP (PSP cohort) were matched to those who did not enroll (non-PSP cohort) based on age, sex, year of treatment initiation, comorbidities, diagnosis, and initiation at a specialty pharmacy. For the PSP cohort, the index date was assigned as the earliest date of PSP enrollment, and time to enrollment following adalimumab initiation was used to assign index dates for the non-PSP cohort. All patients were required to have evidence of medical and pharmacy coverage for at least 6 months before and after their first adalimumab claim and at least 12 months after their index date. Adherence (proportion of days covered during the 12 months following PSP opt-in [index date]) was compared between cohorts using t-tests. Persistence was assessed using survival analysis of discontinuation rates. Medical costs for emergency department, inpatient, physician, and outpatient visits (all-cause and disease-related) and total costs (medical plus drug costs) were compared at 12 months following the index date using t-tests.
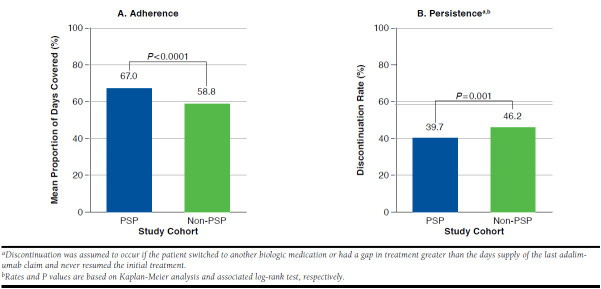
Results: A total of 2,386 patients were included in the study and were allocated to the PSP (n = 1,199) and non-PSP (n = 1,187) cohorts. Baseline characteristics were similar between cohorts. During the follow-up period, adalimumab adherence was 14% greater in the PSP cohort than for the non-PSP cohort (67.0% vs. 58.8%; P < 0.001). The discontinuation rate for adalimumab was 14% lower in the PSP cohort compared with the non-PSP cohort (39.7% vs. 46.2%; P = 0.001). Univariate analyses showed that PSP patients had 23% lower 12-month medical costs (excluding costs for biologic treatment) than did non-PSP patients ($18,322 vs. $23,679; P = 0.003). Disease-related medical costs were 22% lower for PSP than for non-PSP patients ($8,001 vs. $10,202; P = 0.045). Total costs were 10% lower for PSP than for non-PSP patients ($35,741 vs. $39,713; P = 0.030).
Conclusions: Patient enrollment in the PSP was associated with greater adherence, improved persistence, and reduced medical (all-cause and disease-related) and total health care costs for patients receiving adalimumab therapy.
Disclosures: Design, study conduct, and financial support for this study were provided by AbbVie. AbbVie participated in the interpretation of data, review, and approval of the abstract. All authors contributed to the development of the publication and maintained control over the final content. Rubin has received consulting fees or research support from AbbVie, Amgen, Emmi, Genentech, Ironwood, Janssen, Pfizer, Prometheus, Shire, and Takeda. Skup and Mittal are employees and stockholders of AbbVie. Chao was an employee of AbbVie at the time of the study and may hold AbbVie stock. Johnson and Davis are employees of Medicus Economics, which received payment from AbbVie to participate in this research. Study concept and design were contributed by Rubin, Mittal, Chao, and Skup, along with Davis and Johnson. Davis and Johnson took the lead in data collection, with assistance from the other authors, and data interpretation was performed by Rubin, Mittal, Chao, and Skup, with assistance from Davis and Johnson. All authors contributed to the writing and revision of the manuscript. The abstract for this study was published as Rubin DT, Skup M, Davis M, Johnson S, Chao J. Impact of AbbVie's patient support program on resource costs in Crohn's disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, and ankylosing spondylitis. J Manag Care Spec Pharm. 2015;21(Suppl 4a):S74-75 (poster presentation at Academy of Managed Care, 27th Annual Meeting and Expo; April 7-10, 2015; San Diego, CA) and as abstract 2339 in Arthritis Rheumatol. 2015;67(Suppl 10; poster presentation at American College of Rheumatology 2015 ACR/AHRP Annual Meeting; November 7-11, 2015; San Francisco, CA).
Conflict of interest statement
Design, study conduct, and financial support for this study were provided by AbbVie. AbbVie participated in the interpretation of data, review, and approval of the abstract. All authors contributed to the development of the publication and maintained control over the final content. Rubin has received consulting fees or research support from AbbVie, Amgen, Emmi, Genentech, Ironwood, Janssen, Pfizer, Prometheus, Shire, and Takeda. Skup and Mittal are employees and stockholders of AbbVie. Chao was an employee of AbbVie at the time of the study and may hold AbbVie stock. Johnson and Davis are employees of Medicus Economics, which received payment from AbbVie to participate in this research.
Study concept and design were contributed by Rubin, Mittal, Chao, and Skup, along with Davis and Johnson. Davis and Johnson took the lead in data collection, with assistance from the other authors, and data interpretation was performed by Rubin, Mittal, Chao, and Skup, with assistance from Davis and Johnson. All authors contributed to the writing and revision of the manuscript.
The abstract for this study was published as Rubin DT, Skup M, Davis M, Johnson S, Chao J. Impact of AbbVie’s patient support program on resource costs in Crohn’s disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, and ankylosing spondylitis.
Figures
References
-
- Feldmann M. Development of anti-TNF therapy for rheumatoid arthritis. Nat Rev Immun. 2002;2(5):364-71. - PubMed
-
- Maini R, St Clair EW, Breedveld F, et al. . Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT Study Group. Lancet. 1999;354(9194):1932-39. - PubMed
-
- Sandborn WJ, Hanauer S, Loftus EV Jr, et al. . An open-label study of the human anti-TNF monoclonal antibody adalimumab in subjects with prior loss of response or intolerance to infliximab for Crohn’s disease. Am J Gastroenterol. 2004;99(10):1984-89. - PubMed
-
- van der Heijde D, Sieper J, Maksymowych WP, et al. . 2010 Update of the international ASAS recommendations for the use of anti-TNF agents in patients with axial spondyloarthritis. Ann Rheum Dis. 2011;70(6):905-08. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
