

Impact of ischemic preconditioning on surgical treatment of brain tumors: a single-center, randomized, double-blind, controlled trial
- PMID: 28738862
- PMCID: PMC5525340
- DOI: 10.1186/s12916-017-0898-1
Impact of ischemic preconditioning on surgical treatment of brain tumors: a single-center, randomized, double-blind, controlled trial
Abstract
Background: Postoperative ischemia is a frequent phenomenon in patients with brain tumors and is associated with postoperative neurological deficits and impaired overall survival. Particularly in the field of cardiac and vascular surgery, the application of a brief ischemic stimulus not only in the target organ but also in remote tissues can prevent subsequent ischemic damage. We hypothesized that remote ischemic preconditioning (rIPC) in patients with brain tumors undergoing elective surgical resection reduces the incidence of postoperative ischemic tissue damage and its consequences.
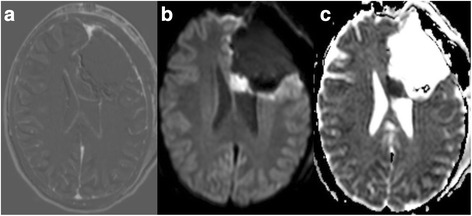
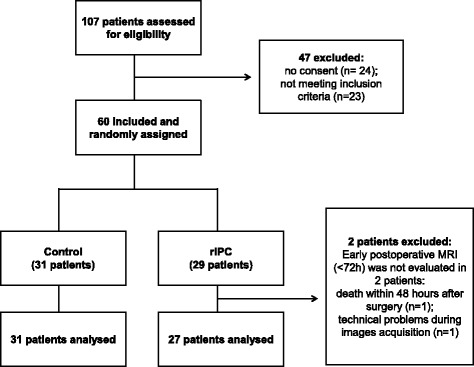
Methods: Sixty patients were randomly assigned to two groups, with 1:1 allocation, stratified by tumor type (glioma or metastasis) and previous treatment with radiotherapy. rIPC was induced by inflating a blood pressure cuff placed on the upper arm three times for 5 min at 200 mmHg in the treatment group after induction of anesthesia. Between the cycles, the blood pressure cuff was released to allow reperfusion. In the control group no preconditioning was performed. Early postoperative magnetic resonance images (within 72 h after surgery) were evaluated by a neuroradiologist blinded to randomization for the presence of ischemia and its volume.
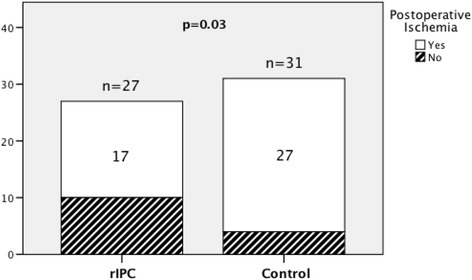
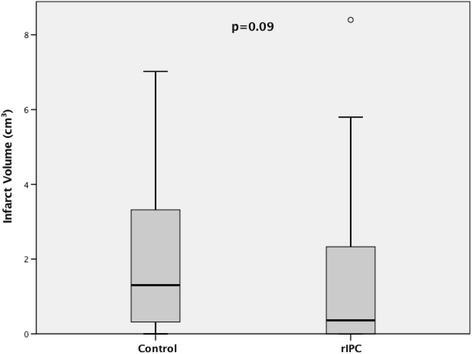
Results: Fifty-eight of the 60 patients were assessed for occurrence of postoperative ischemia. Of these 58 patients, 44 had new postoperative ischemic lesions. The incidence of new postoperative ischemic lesions was significantly higher in the control group (27/31) than in the rIPC group (17/27) (p = 0.03). The median infarct volume was 0.36 cm3 (interquartile range (IR): 0.0-2.35) in the rIPC group compared with 1.30 cm3 (IR: 0.29-3.66) in the control group (p = 0.09).
Conclusions: Application of rIPC was associated with reduced incidence of postoperative ischemic tissue damage in patients undergoing elective brain tumor surgery. This is the first study indicating a benefit of rIPC in brain tumor surgery.
Trial registration: German Clinical Trials Register, DRKS00010409 . Retrospectively registered on 13 October 2016.
Keywords: Brain metastasis; Brain tumor; Glioma; Ischemic preconditioning; Neurooncology; Neurosurgery; Stroke.
Conflict of interest statement
Ethics approval and consent to participate
The medical ethics committee of the Technical University of Munich approved all the experiments described in this study. We have obtained written informed consent from all patients included in this study. Patients may cancel their participation at any time upon request.
Consent for publication
Not applicable.
Competing interests
Stefanie Bette, Jens Gempt and Bernhard Meyer work as consultants for Brainlab (Brainlab AG, Feldkirchen, Germany).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Hausenloy DJ, Mwamure PK, Venugopal V, Harris J, Barnard M, Grundy E, et al. Effect of remote ischaemic preconditioning on myocardial injury in patients undergoing coronary artery bypass graft surgery: a randomised controlled trial. Lancet. 2007;370:575–9. doi: 10.1016/S0140-6736(07)61296-3. - DOI - PubMed
-
- McCrindle BW, Clarizia NA, Khaikin S, Holtby HM, Manlhiot C, Schwartz SM, et al. Remote ischemic preconditioning in children undergoing cardiac surgery with cardiopulmonary bypass: a single-center double-blinded randomized trial. J Am Heart Assoc. 2014;3 doi: 10.1161/JAHA.114.000964. - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
