

Temporal Trends and Factors Associated with Home Hemodialysis Technique Survival in Canada
- PMID: 28739576
- PMCID: PMC5544522
- DOI: 10.2215/CJN.13271216
Temporal Trends and Factors Associated with Home Hemodialysis Technique Survival in Canada
Abstract
Background and objectives: The last 15 years has seen growth in home hemodialysis (HD) utilization in Canada owing to reports of improved outcomes relative to patients on conventional in-center HD. What effect growth has had on home HD technique and patient survival during this period is not known.
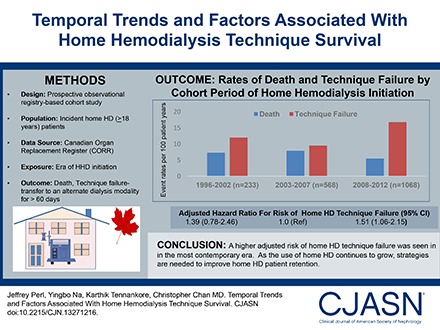
Design, settings, participants, & measurements: We compared the risk of home HD technique failure, mortality, and the composite outcome among three incident cohorts of patients on home HD in Canada: 1996-2002, 2003-2007, and 2008-2012. A multivariable piece-wise exponential model was used to evaluate all outcomes using inverse probability of treatment and censoring weights.
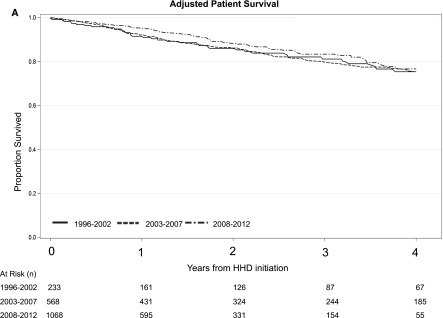
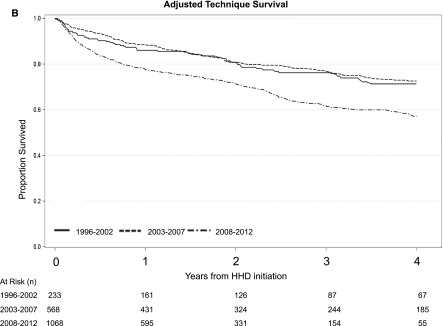
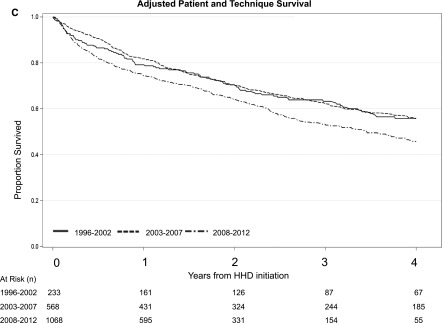
Results: A total of 1869 incident patients on home HD were identified from the Canadian Organ Replacement Register. Relative to those treated between 2003 and 2007 (n=568), the risk of home HD technique failure was similar between patients treated between 1996 and 2002 (n=233; adjusted hazard ratio [AHR], 1.39; 95% confidence interval [95% CI], 0.78 to 2.46) but higher among incident patients on home HD treated between 2008 and 2012 (n=1068; AHR, 1.51; 95% CI, 1.06 to 2.15). Relative to patients treated between 2003 and 2007, adjusted mortality was similar among those treated between 2008 and 2012 (AHR, 0.83; 95% CI, 0.58 to 1.19) and those treated between 1996 and 2002 (AHR, 0.67; 95% CI, 0.38 to 1.21). The risk of the composite outcome of death and technique failure was similar across cohorts, as was the risk of receiving a kidney transplant. Increasing age, diabetes as a comorbidity, and smoking status were associated with an increased risk of death as well as the composite outcome. Medium-sized facilities had a lower risk of death, technique failure, and the composite outcome compared with larger facilities.
Conclusions: A higher risk of technique failure was seen in the most contemporary era. Further characterization of the risk factors for, and causes of technique failure is needed to develop strategies to improve patient retention on home HD.
Keywords: Canada; Canadian Organ Replacement Register; Comorbidity; Death; Dialysis Modality Discontinuation; Hemodialysis; Hemodialysis, Home; Home Dialysis Discontinuation; Humans; Proportional Hazards Models; Smoking; Technique Failure; diabetes mellitus; home hemodialysis; kidney transplantation; risk factors; short daily hemodialysis; slow nocturnal hemodialysis; survival; technique survival.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Maintaining Patients on Home Hemodialysis: The Journey Matters as Does the Destination.Clin J Am Soc Nephrol. 2017 Aug 7;12(8):1209-1211. doi: 10.2215/CJN.06890617. Epub 2017 Jul 24. Clin J Am Soc Nephrol. 2017. PMID: 28739574 Free PMC article. No abstract available.
References
-
- Canadian Organ Replacement Register: Preliminary Statistics for Renal Failure and Solid Organ Transplantation in Canada, Ottawa, ON, Canadian Organ Replacement Register, 2015
-
- Jayanti A, Morris J, Stenvinkel P, Mitra S: Home hemodialysis: Beliefs, attitudes, and practice patterns. Hemodial Int 18: 767–776, 2014 - PubMed
-
- Culleton BF, Walsh M, Klarenbach SW, Mortis G, Scott-Douglas N, Quinn RR, Tonelli M, Donnelly S, Friedrich MG, Kumar A, Mahallati H, Hemmelgarn BR, Manns BJ: Effect of frequent nocturnal hemodialysis vs conventional hemodialysis on left ventricular mass and quality of life: A randomized controlled trial. JAMA 298: 1291–1299, 2007 - PubMed
-
- Chan CT, Floras JS, Miller JA, Richardson RM, Pierratos A: Regression of left ventricular hypertrophy after conversion to nocturnal hemodialysis. Kidney Int 61: 2235–2239, 2002 - PubMed
-
- Walsh M, Culleton B, Tonelli M, Manns B: A systematic review of the effect of nocturnal hemodialysis on blood pressure, left ventricular hypertrophy, anemia, mineral metabolism, and health-related quality of life. Kidney Int 67: 1500–1508, 2005 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
