

Insights in Anaphylaxis and Clonal Mast Cell Disorders
- PMID: 28740494
- PMCID: PMC5502410
- DOI: 10.3389/fimmu.2017.00792
Insights in Anaphylaxis and Clonal Mast Cell Disorders
Abstract
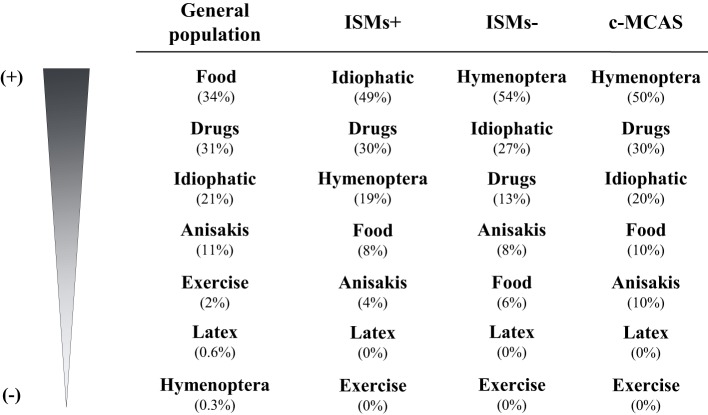
The prevalence of anaphylaxis among patients with clonal mast cell disorders (MCD) is clearly higher comparing to the general population. Due to a lower frequency of symptoms outside of acute episodes, clonal MCD in the absence of skin lesions might sometimes be difficult to identify which may lead to underdiagnosis, and anaphylaxis is commonly the presenting symptom in these patients. Although the release of mast cell (MC) mediators upon MC activation might present with a wide variety of symptoms, particular clinical features typically characterize MC mediator release episodes in patients with clonal MCD without skin involvement. Final diagnosis requires a bone marrow study, and it is recommended that this should be done in reference centers. In this article, we address the main triggers for anaphylaxis, risk factors, clinical presentation, diagnosis, and management of patients with MC activation syndromes (MCASs), with special emphasis on clonal MCAS [systemic mastocytosis and mono(clonal) MC activations syndromes].
Keywords: anaphylaxis; clonal; mast cell; mast cell activation syndrome; mastocytosis.
Figures
References
-
- Sampson HA, Munoz-Furlong A, Campbell RL, Adkinson NF, Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report – Second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network symposium. J Allergy Clin Immunol (2006) 117(2):391–7.10.1016/j.jaci.2005.12.1303 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources