

Salvage Embolization and Histologic Analysis of Gastric Cancer with Hemorrhagic Shock Using Spherical Embolic Material
- PMID: 28740566
- PMCID: PMC5507799
- DOI: 10.12659/PJR.901602
Salvage Embolization and Histologic Analysis of Gastric Cancer with Hemorrhagic Shock Using Spherical Embolic Material
Abstract
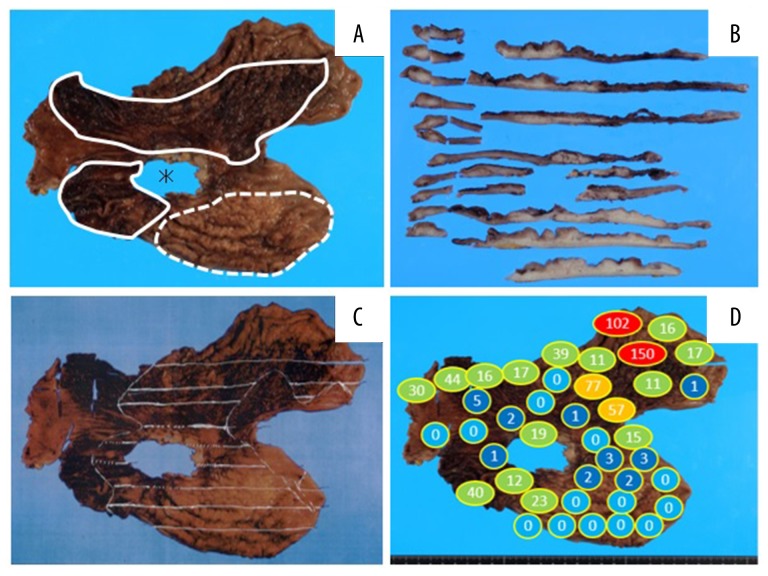
Background: In a recent study, it was reported that transcatheter arterial embolization with spherical embolic material for life-threatening hemorrhages in various cancer patients was safe and effective. Calibrated microspheres are able to access distal regions of the target arteries, which results in the disappearance of tumor staining. However, there are few reports on the pathological behavior of EmboSpheres in gastric cancer specimens. In this case, we succeeded in salvage embolization for advanced gastric cancer with hemorrhagic shock using spherical embolic material. To our knowledge, this is the first report of a pathological evaluation of spherical embolic microspheres in a gastric cancer specimen.
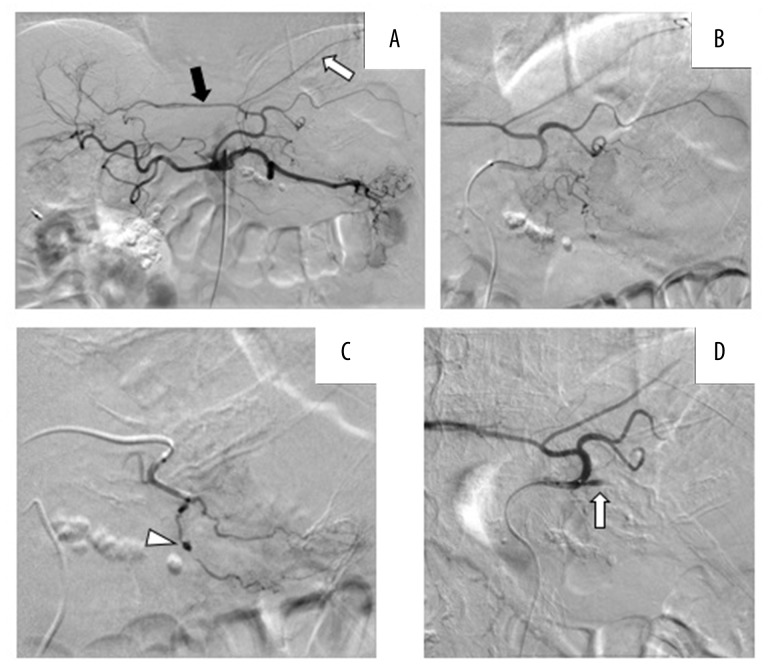
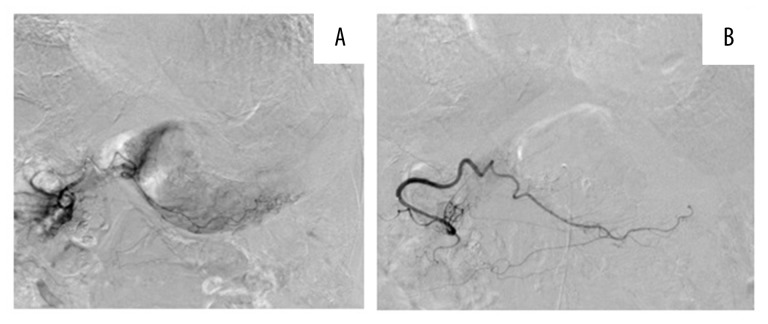
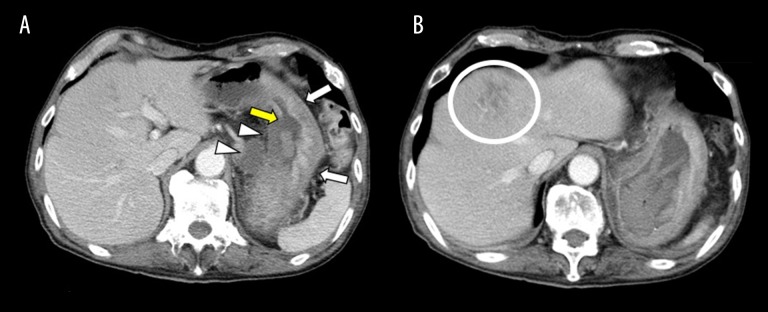
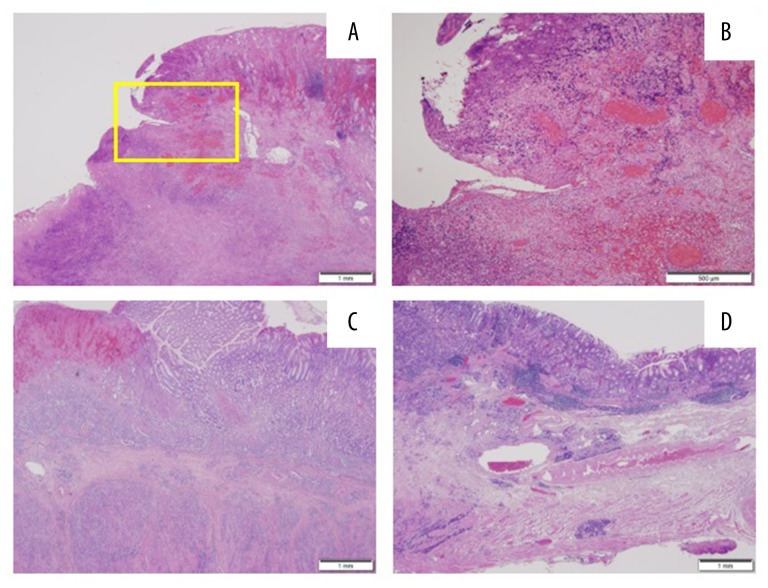
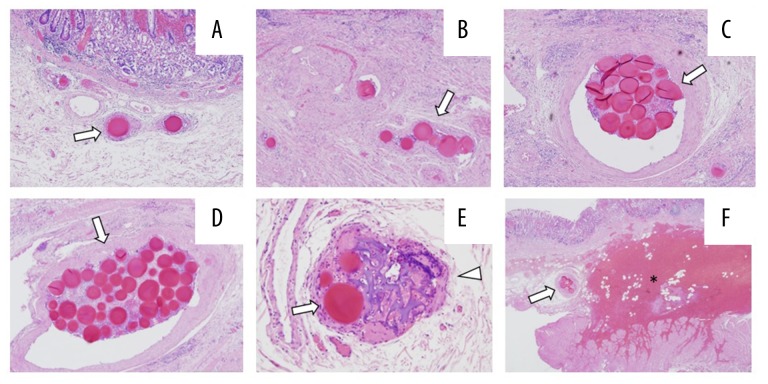
Case report: A 70-year-old man with scirrhous gastric cancer was admitted to our hospital for staging laparoscopy. Unfortunately, he had a sudden onset of hematemesis and melena leading to hemorrhagic shock due to bleeding from the gastric cancer. While undergoing a rapid blood transfusion, he underwent emergent embolization to achieve hemostasis. The left gastric and right gastroepiploic arteries were embolized with spherical embolic material, and the patient survived. Two days later, the patient was able to undergo gastrectomy. A large number of microspheres were observed in areas of hemorrhage. The range and median diameter of the minor axis were 177-1048 μm and 281 μm, respectively.
Conclusions: Transcatheter arterial embolization using spherical embolic material could become one of safe and effective options, especially when there is no extravasation or pseudoaneurysm but only tumor staining from the clinical and pathological point of view.
Keywords: Catheterization, Peripheral; Embolization, Therapeutic; Hemostasis; Microspheres; Stomach Neoplasms.
Figures

References
-
- Lee HH, Park JM, Chun HJ, et al. Transcatheter arterial embolization for endoscopically unmanageable non-variceal upper gastrointestinal bleeding. Scand J Gastroenterol. 2015;50(7):809–15. - PubMed
-
- So JBY, Yam A, Cheah WK, et al. Risk factors related to operative mortality and morbidity in patients undergoing emergency gastrectomy. Br J Surg. 2000;87(12):1702–7. - PubMed
-
- Loffroy R, Rao P, Ota S, et al. Embolization of acute nonvariceal upper gastrointestinal hemorrhage resistant to endoscopic treatment: Results and predictors of recurrent bleeding. Cardiovasc Intervent Radiol. 2010;33(6):1088–100. - PubMed
-
- Koh KH, Kim K, Kwon DH, et al. The successful endoscopic hemostasis factors in bleeding from advanced gastric cancer. Gastric Cancer. 2013;16(3):397–403. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources