

Effectiveness of perioperative pulmonary rehabilitation in thoracic surgery
- PMID: 28740672
- PMCID: PMC5506174
- DOI: 10.21037/jtd.2017.05.49
Effectiveness of perioperative pulmonary rehabilitation in thoracic surgery
Abstract
Background: Functional condition is crucial for operability of patients with lung cancer and/or chronic respiratory diseases. The aim of the study was to measure changes of functional and quality of life parameters in terms of the effectiveness of perioperative pulmonary rehabilitation (PR).
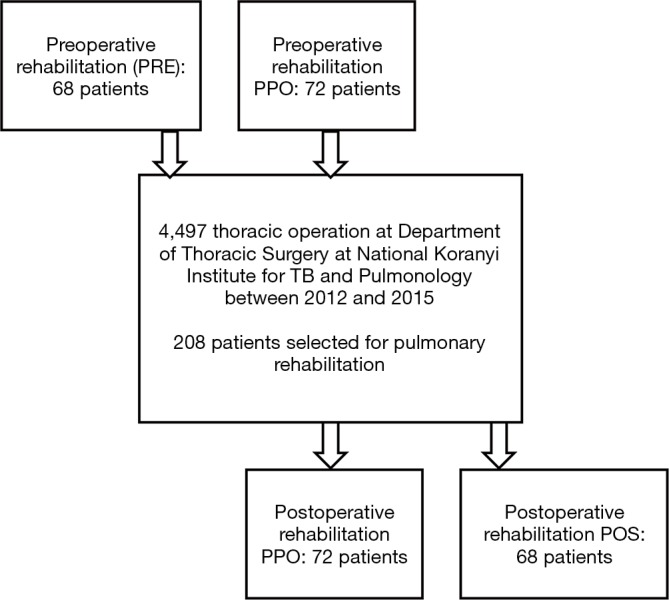
Methods: A total of 208 COPD patients (age: 63±9 years, man/woman: 114/94, FEV1: 62±14%pred) participated in a perioperative PR program. The indication was primary lung cancer in 72% of the patients. The 68 patients participated in preoperative (PRE) rehabilitation, 72 in a pre- and postoperative rehabilitation (PPO) and 68 patients only in postoperative rehabilitation (POS). PR program included respiratory training techniques, individualized training and smoking cessation. Lung function tests, 6 minutes walking distance (6MWD) were measured before and after the rehabilitation. Quality of life tests [COPD Assessment Test (CAT) and Modified Medical Research Council Dyspnoea Scale (mMRC)] were evaluated as well.
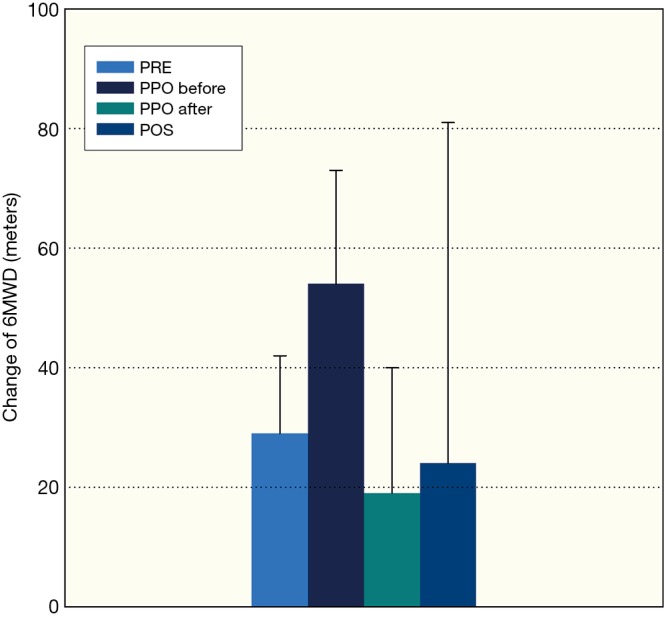
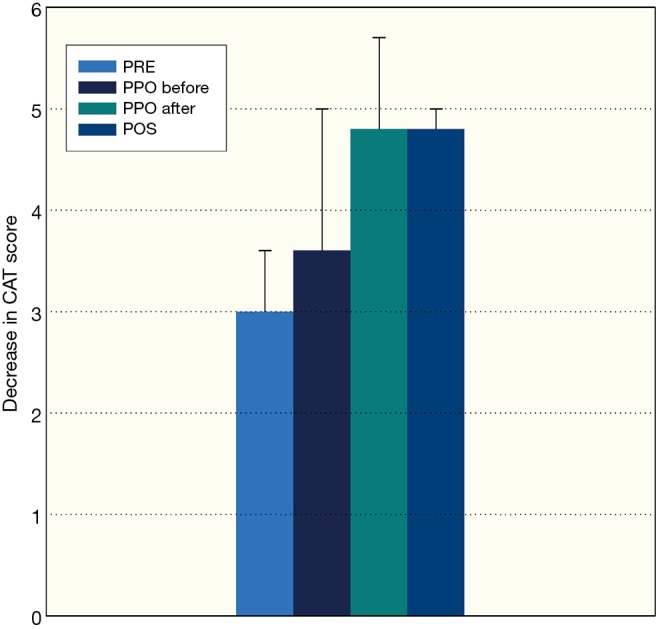
Results: There was a significant improvement in FEV1 (PRE: 64±16 vs. 67±16%pred; PPO: 60±13 vs. 66±13%pred before the operation, 48±13 vs. 52±13%pred after the operation; POS: 56±16 vs. 61±14%pred, P<0.05) and 6MWD (PRE: 403±87 vs. 452±86 m; PPO: 388±86 vs. 439±83 m before, 337±111 vs. 397±105 m after the operation; POS: 362±89 vs. 434±94 m, P<0 0001). Significant improvement was detected in FVC, grip strength, mMRC and CAT questionnaires as an effectiveness of PR, also. Average intensive care duration was 3.8±5.2 days with vs. 3.1±3.6 without preoperative PR.
Conclusions: Improvements in exercise capacity and quality of life were seen following PR both before and after thoracic surgery.
Keywords: Perioperative pulmonary rehabilitation (perioperative PR); chest physiotherapy; chronic obstructive pulmonary disease (COPD); endurance training; lung cancer; thoracic surgery.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
References
-
- Brunelli A, Charloux A, Bolliger CT, et al. European Respiratory Society; European Society of Thoracic Surgeons Joint Task Force on Fitness For Radical Therapy. The European Respiratory Society and European Society of Thoracic Surgeons clinical guidelines for evaluating fitness for radical treatment (surgery and chemoradiotherapy) in patients withlung cancer. Eur J Cardiothorac Surg 2009;36:181-4. 10.1016/j.ejcts.2009.04.022 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous