

Pediatric airway surgery
- PMID: 28740684
- PMCID: PMC5506117
- DOI: 10.21037/jtd.2017.05.50
Pediatric airway surgery
Abstract
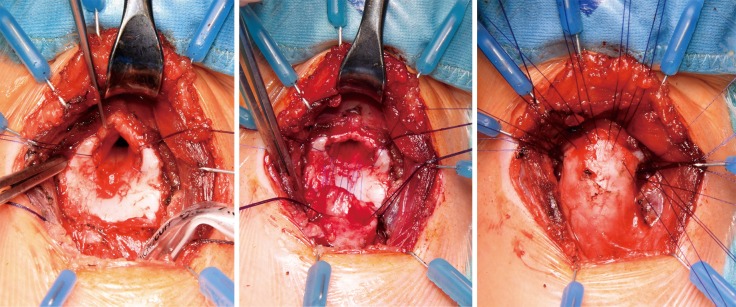
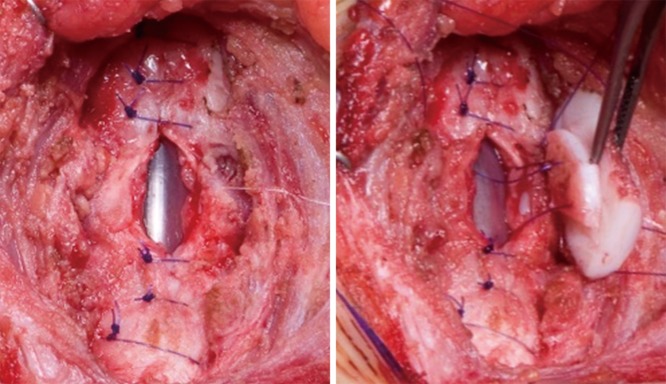
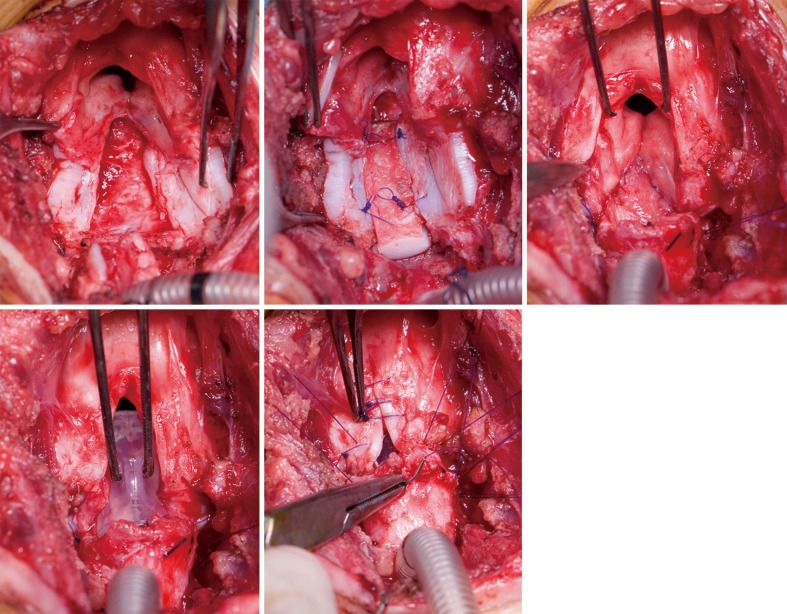
The management of pediatric airway pathology can be challenging and requires a dedicated team, consisting of thoracic surgeons, phoniatricians, logopedics, pediatricians and anesthetists. It necessitates a tailored treatment approach for each individual patient in order to address the minor variances that exist between cases. The majority of pediatric airway problems are a sequela of prematurity and prolonged post-partal intubation/tracheostomy. Surgical repair is often complicated by additional malformation or severe comorbidities. This comprehensive review should give an overview on most common airway problems in neonates and children as well as available surgical techniques.
Keywords: Pediatric; airway; stenosis; surgical techniques.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures


References
-
- Monnier P. Pediatric airway surgery management of laryngotracheal stenosis in infants and children. 2011:xvii, 371 p.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources