

Whole lung lavage-technical details, challenges and management of complications
- PMID: 28740686
- PMCID: PMC5506114
- DOI: 10.21037/jtd.2017.04.10
Whole lung lavage-technical details, challenges and management of complications
Abstract
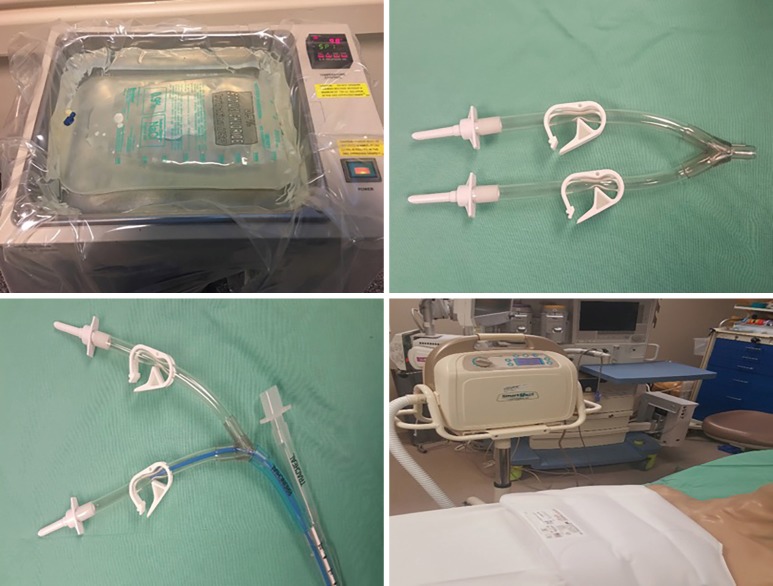
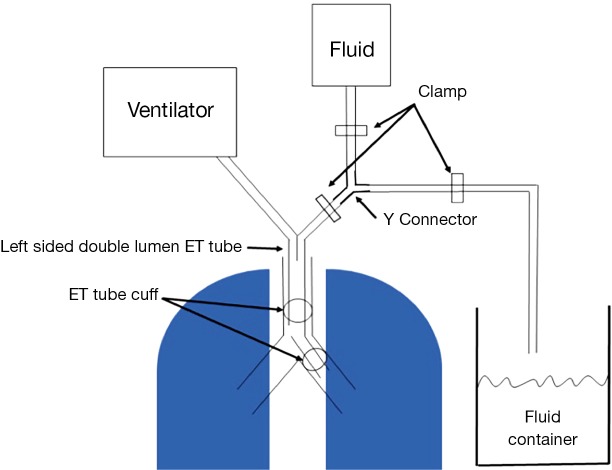
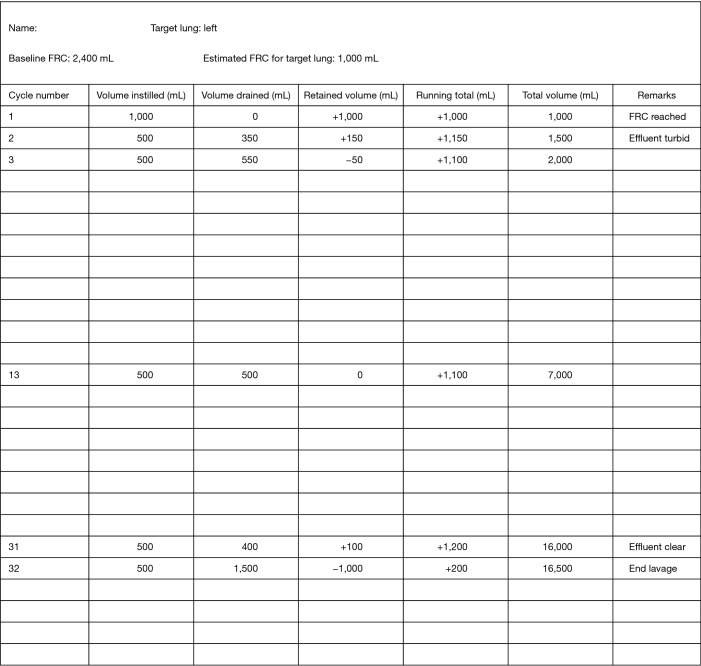
Pulmonary alveolar proteinosis (PAP) is a rare disease characterized by alveolar accumulation of surfactant material with resulting hypoxemia and reduced lung function. Whole lung lavage (WLL) to physically remove the proteinaceous material from the affected lung is the standard treatment. Since its original description in 1964, there have been increasing numbers of WLL procedures done worldwide and the technique has been variously refined and modified. When done in experienced centers, WLL provides long lasting benefit in the majority of patients. It is considered safe and effective. There are no guidelines standardizing the procedure. Our preferred method is to lavage one lung at a time, with the patient supine, filling to functional residual capacity (FRC) and repeating cycles of drainage and instillation with chest percussion until the effluent is clear. The aim of this article is to provide a detailed description of the technique, equipment needed and logistic considerations as well as providing a physiologic rationale for each step of WLL. We will also review the available data concerning variations of the technique described in the literature.
Keywords: Pulmonary alveolar proteinosis (PAP); rare disease; whole lung lavage (WLL).
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

References
-
- De Sanctis PN. Pulmonary alveolar proteinosis. A review of the findings and theories to date, with a digression on Pneumocystis carinii pneumonia. BMQ 1962;13:19-35. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials