

Multimodality imaging assessment of mitral valve anatomy in planning for mitral valve repair in secondary mitral regurgitation
- PMID: 28740719
- PMCID: PMC5505945
- DOI: 10.21037/jtd.2017.06.99
Multimodality imaging assessment of mitral valve anatomy in planning for mitral valve repair in secondary mitral regurgitation
Abstract
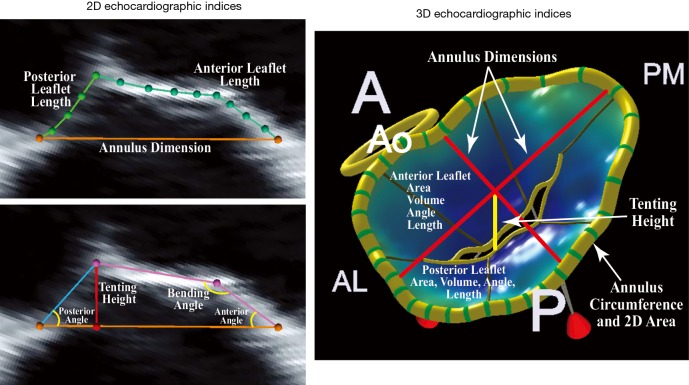
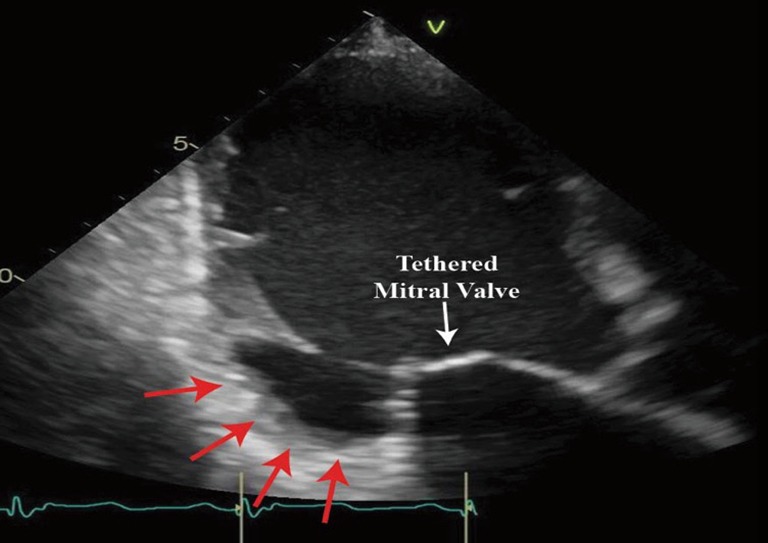
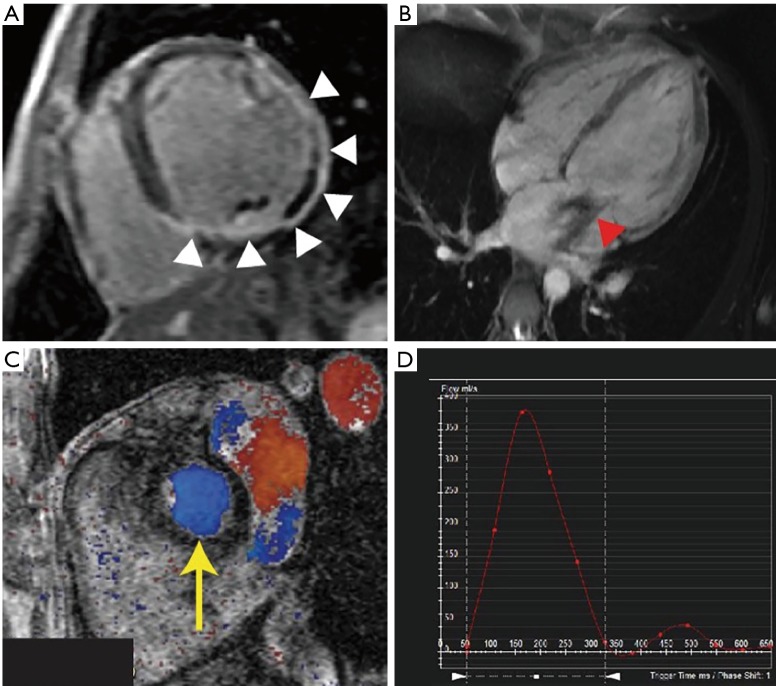
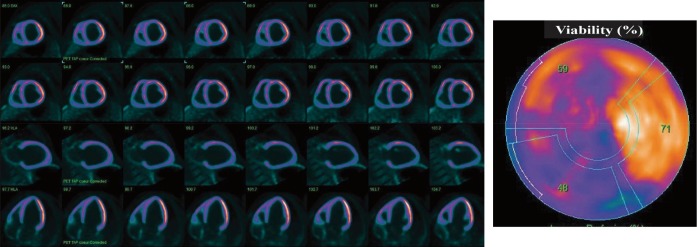
Secondary mitral regurgitation (MR) is frequent valvular heart disease and conveys worse prognostic. Therapeutic surgical or percutaneous options are available in the context of severe symptomatic secondary MR, but the best approach to treat these patients remains unclear, given the lack of clear clinical evidence of benefit. A comprehensive evaluation of the mitral valve apparatus and the left ventricle (LV) has the ability to clearly define and characterize the disease, and thus determine the best option for the patient to improve its clinical outcomes, as well as quality of life and symptoms. The current report reviews the mitral valve (MV) anatomy, the underlying mechanisms associated with secondary MR, the related therapeutic options available, and finally the usefulness of a multimodality imaging approach for the planning of surgical or percutaneous mitral valve intervention.
Keywords: Secondary mitral regurgitation; cardiac magnetic resonance (CMR); computed tomography (CT); echocardiography; multimodality imaging; positron emission tomography (PET).
Conflict of interest statement
Conflicts of Interest: N Piriou has served as consultant for Abbott Vascular and has received fees. The other authors have reported no relationship to disclose.
Figures




References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources